
Cranial ultrasound: a guideline for the performance of routine cranial USS for preterm infants
Objectives
This Guideline is applicable to medical staff and ANNPs caring for neonates in the West of Scotland. All staff performing cranial ultrasound scans on neonates must first ensure that they have received training in the correct use of the ultrasound scanner and the appropriate images required, as outlined in this document. Except in an emergency, parents should be informed in advance that head scans will be performed on their baby, and the reasons for this. This information may be given verbally or in a printed form. The results of the scans should be communicated in a timely manner by a senior member of staff able to interpret the images and understand their prognostic value.
This document will primarily cover standard cranial ultrasound techniques for recording peri-ventricular haemorrhage (PVH) and peri-ventricular leucomalacia (PVL), including the measurement of the resistive index and ventricular dilatation.
Cranial ultrasonography is the most widely used neuroimaging procedure in the neonatal period. It plays a central role in the detection and management of some neonatal neurological disease and can provide prognostic, as well as diagnostic, information to neonatologists. This guideline provides a standard for clinicians in order to detect abnormalities that will alter management and/or guide parental counselling.
There are a diverse group of infants who will require scanning and ultimately a decision to perform a scan on any unwell neonate can be taken by the consultant responsible for that child. Common indications include:
- Premature infants
- Infants with neurological abnormalities e.g. seizures
- Infants with antenatally detected abnormalities eg ventriculomegaly
- Infants with hypoxic ischaemic encephalopathy
- Infants with other congenital abnormalities
- Infants with congenital or acquired CNS infection
- Infants with a diagnosis of coagulopathy or thrombocytopenia
For auditing purposes it is necessary to store an adequate series of images for later review. This is of particular importance for the benchmarking scans, for the diagnosis of the maximum grade of PVH and the presence or absence of cystic PVL.
|
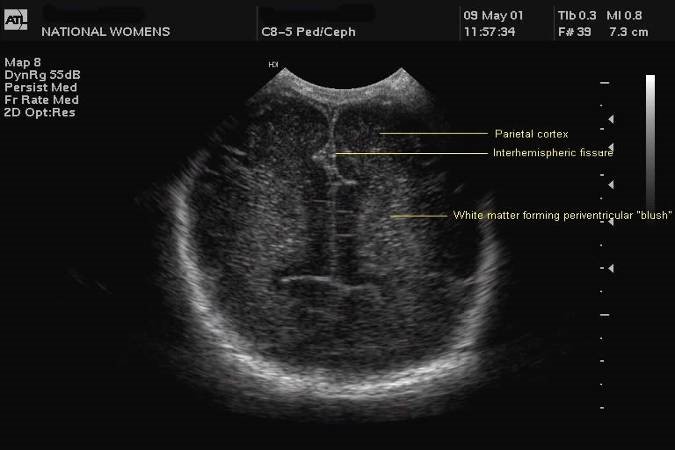
Coronal plane (6+ images)
|
 |
|
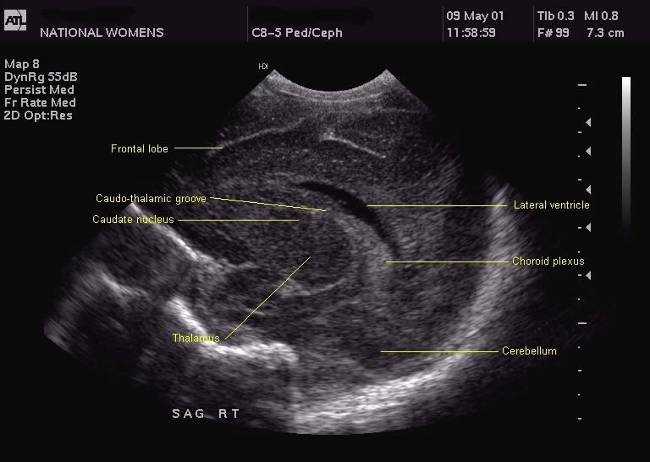
Sagittal plane (5+ images)
When there is evidence of Hypoxic Ischaemic Encephalopathy (HIE) or ventricular dilatation, the resistance index should be measured using the mid-sagittal plane. The anterior cerebral artery is identified with colour Doppler at its vertical course, immediately anterior to the genu of the corpus callosum |
 |
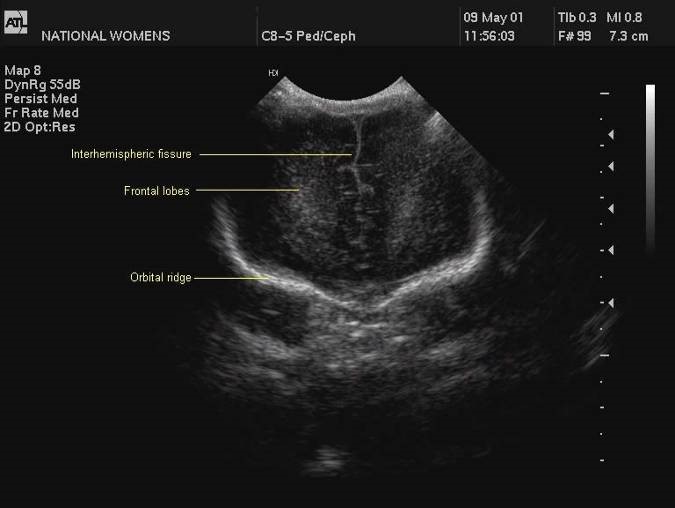
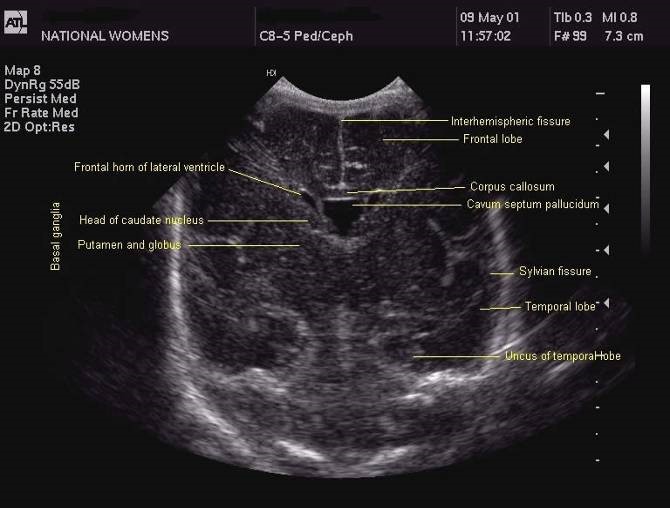
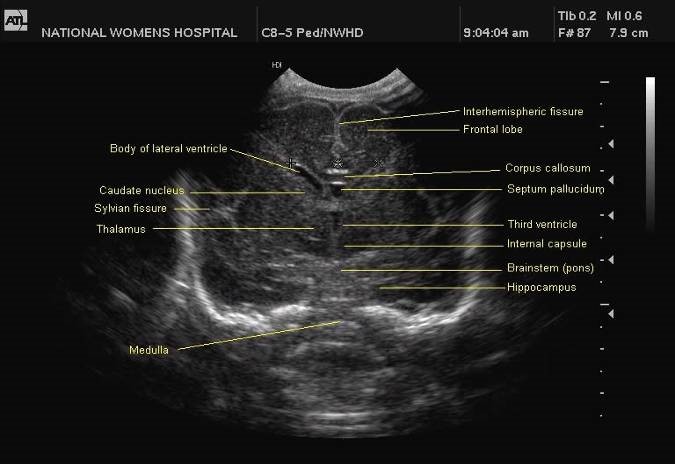
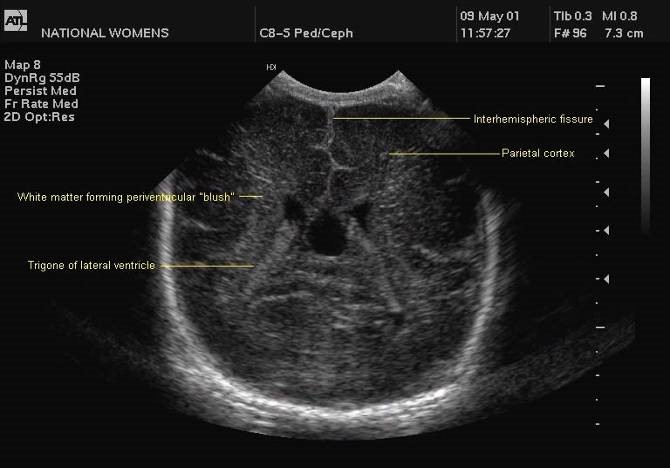
See sample images below (click on image to display larger size):
 |
 |
 |
 |
 |
 |
 |
 |
The following routine scans should be performed for all infants less than 32 weeks gestation:
|
Day 1 |
For detection of periventricular haemorrhage |
|
|
Day 28 |
For detection of periventricular leucomalacia |
Additional scans should be performed as clinically indicated.
For detection of Periventricular Haemorrhage (PVH)
- Routine Scans performed by neonatal staff - Day 1, Day 3, Day 7. The D1 scan should be performed as soon as possible after birth to detect any lesions that may be antenatal in origin. However this should be deferred if there is any concern that a CrUSS at that point could destabilise the patient.
- Benchmarking Scan – To define maximum grade of PVH for Badger.
Where radiology input is available this should be booked for the 1st radiology visit between Day 7 – 14. Otherwise the Day 7 routine scan should be utilised - Clinical staff responsible for the baby should ensure that all of the above scans are entered into Badger, using the categorisation in the badger database.
Monitoring of babies at risk of Post-haemorrhagic Ventricular dilatation (PHVD)
All babies who are diagnosed with PVH and any infant whose routine measurements of OFC increase across centile lines should have further scans to monitor for evidence of PHVD
- Neonatal Staff – Additional USS scans are required in the 2nd-3rd week of life following a diagnosis of PVH. The frequency of these scans will be determined based on the severity of PVH and any indication of the development of PVHD.
A single scan should be considered in any infant whose OFC crosses centile lines on routine monitoring - Radiology – Where possible, a formal radiology scan should ideally be performed in any infant in whom a ventricular drainage procedure is being considered. This may require the transfer of the infant to a tertiary level unit.
Exceptions are necessary where there is acute symptomatology outside normal radiology sessions.
For detection of Periventricular Leucomalacia (PVL)
- Routine scan performed by Neonatal staff – Day 28 or shortly thereafter.
- Benchmarking Scan – To define the presence or absence of cystic PVL for Badger
Where radiology input is available this should be ordered on day 28 to be performed between 28 days and discharge. Otherwise the Day 28 scan should be utilised
All scans must be performed, or supervised, by a clinician with sufficient experience to ensure the quality of the images produced and their interpretation. This would usually be a career grade paediatrician with an interest in neonatology, or, a senior neonatal trainee. Less experienced trainees must be supervised until this standard is achieved. Neonatal trainees should be encouraged to attend a formal training course.
Level 3 units should consider seeking formal radiology input, for the benchmarking scans, where this is not currently available.
PVH may be asymptomatic and without long term consequence. There is a strong association between extensive PVH and early neonatal mortality, neurodevelopmental disability and post haemorrhagic hydrocephalus. Most observers agree that the more severe grades of haemorrhage are associated with a higher incidence of neuro-developmental handicap.
Appendix 1 provides estimates for the incidence of neurodevelopmental handicap with different severities of PVH
A full description of the findings should be entered in the notes and, for the purposes of data collection and benchmarking, PVH should be graded using the same system used by the Vermont Oxford Network:
- Grade 0: No subependymal or intraventricular haemorrhage
- Grade 1: Subependymal germinal matrix haemorrhage only
- Grade 2: Intraventricular blood, no ventricular dilation
- Grade 3: Intraventricular blood, ventricular dilation
- Grade 4: Intraparenchymal haemorrhage
NB – for Grade 3 PVH, the dilatation of the ventricle refers to dilatation due to the volume of intraventricular blood. Dilatation of the ventricle due to CSF (Post Haemorrhagic Ventricular Dilatation - PVHD) should be recorded as an additional finding.
Mild degrees of PVL may result in transient periventricular echodensities or mild enlargement of the lateral ventricles. These changes are not associated with a significant increase in neurodevelopmental handicap. It is therefore important that serial cranial ultrasound scans are performed within the above timeframe to ensure that any echodensities noted are assessed for either improvement or development of cystic PVL. With cystic PVL, the risks of neurodevelopmental handicap are significantly increased as outlined in Appendix 1. The risk of handicap also increases with more extensive and bilateral changes.
For the purposes of data collection and benchmarking PVL should be diagnosed only in the presence of cystic PVL.
NB – It is common to find benign periventricular cysts on routine cranial scans. It is important not to mistake these for cystic PVL or porencephaly. The diagram below indicates the typical locations of of each type of periventricular cyst
 |
If cysts are seen around the lateral ventricles, it is important to determine their position in regard to the upper part of the lateral ventricle. 1+2 = Germinolytic cysts and Pseudocysts are below or at the level of the upper part of the lateral ventricle. 3 = Cystic periventricular leukomalacia is mostly above this level 4 = Cysts as a result of a venous infarct (porencephaly) are large and can be either above, at or below this level |
In addition to routine Cranial USS imaging, as described above, all premature infants should have measurements of their OFC performed weekly to identify cases of Post-haemorrhagic Ventricular Dilatation (PVHD). All babies with PHVD need regular scans to monitor the progression of the ventricular dilatation and to assess the possible requirement for ventricular drainage. A number of measures have been described to monitor ventricular dilatation the most widely used being the ventriculo-cranial ratio (VCR) and the ventricular index (VI). There is no clear advantage to either measure but it is important to use the same measurement in an individual patient to monitor change over time.
Ventriculo-cranial ratio (VCR)
Measurement of the ventricular system needs to be performed on a symmetrical, easily reproducible view. The ventriculo-cranial ratio (VCR) is the ratio of distance between the lateral sides of the ventricles and the biparietal diameter. This is usually expressed as a percentage with a normal value of around 33-36% in a preterm infant. This value is of most use in monitoring the degree of change between successive measurements. An increasing VCR should trigger frequent reassessments with measurements of the cerebral resistive index (see below).

Ventricular Index (VI)
The Ventricular index, as described by Levine, is the absolute distance between the falx and the lateral wall of the anterior horn in the coronal plane at the level of the third ventricle. Values more than 4mm above the 97th centile for gestational age are indicative of significant ventricular dilatation (see chart). A study by Brouwer et al compared early CSF drainage, at a ventricular index of 4 mm above the 97th centile, to drainage beyond this threshold, and showed that early treatment was associated with better development quotient at 2 years and a decreased likelihood of shunt dependence; there was, however, no reduction in the rate of cerebral palsy with early drainage.
 |
 |
Resistive Index (RI)
In 1976, Pourcelot introduced the concept of RI, which is calculated by the following formula: RI = (S-D)/S where S and D stand for systolic and diastolic velocities measured in the cerebral arteries. The infant’s blood pressure and carbon dioxide tension need to be taken into account when measuring the RI as these can affect cerebral blood flow. Variations in the RI demonstrate that cerebral blood flow is not well regulated and are often associated with adverse outcomes. It is important to interpret the RI with caution as cerebral blood flow is always changing due to haemodynamic alterations and there is also considerable inter and intra observer variation.

Interpretation
High RI
A high RI (>0.85) corresponds to low blood flow velocity where vascular resistance is high (eg hydrocephalus). Infants with values higher than this may require ventricular drainage to reduce intracranial pressure.
NB: A high RI must be interpreted with caution in an infant with a PDA as these infants may have a low diastolic velocity due to ductal steal. This will give a high RI value even in infants with normal intracranial pressure.
Low RI
A low Resistive Index corresponds to high blood flow velocity where vascular resistance is low (eg HIE). In normothermic infants, an RI of <0.55 has a positive predictive value for poor neurological outcome of 84% (95% CI 73%, 91%). However in cooled infants the positive predictive value is lower - 60% (95% CI 45%, 74%). (Elstad M et. al,)
Abnormal findings in a preterm cranial ultrasound include:
- Periventricular haemorrhage PVH (sometimes known as intraventricular or germinal matrix haemorrhage)
- Periventricular leucomalacia (PVL)
- Ventricular dilatation
- Hydrocephalus
This is most common in the premature population and usually occurs within the first week of life. The incidence of PVH decreases with increasing gestational age, and is rare beyond 34 weeks gestation because of involution of the vascular germinal matrix. The incidence of PVH in infants with a birthweight <1500 grams is decreasing and is quoted in the literature as anywhere between 15% and 30%. Many infants are asymptomatic and these haemorrhages are found on surveillance sonography.
Aetiology / Risk factors for PVH
General pathogenetic factors may include antepartum, intrapartum and neonatal conditions:
|
Antepartum |
Intrapartum |
Neonatal |
|
Prematurity Lack of antenatal corticosteroids Maternal pre-eclampsia Antepartum haemorrhage Chorioamnionitis |
Low umbilical artery pH Delivery outside a tertiary unit Delivery mode (C-section protective) Low 1 minute Apgar Bruising at delivery |
Hyaline membrane disease Patent ductus arteriosus Pneumothorax |
Pathogenesis
Crucial to the understanding of the pathogenesis of intraventricular haemorrhage is the concept of impaired autoregulation of cerebral blood flow in the distressed fetus and newborn. Most PVH is secondary to hypoxic ischaemic reperfusion injury of the germinal matrix. In premature infants the germinal matrix is richly perfused with fragile vessels which are particularly vulnerable to insult. Cerebrovascular autoregulation may be absent in sick preterm infants and a patent ductus arteriosus may also ‘steal’ blood from the cerebral circulation. Iatrogenic disturbances in intravascular volume and intrinsic disturbances in coagulation are also associated with an increase in minor grades of PVH. A large periventricular haemorrhage can result in a venous haemorrhagic infarct secondary to the obstruction of drainage.
Interventions
Only a limited number of interventions have been demonstrated to alter the risk of PVH: Maternal transfer to a tertiary neonatal centre; Antenatal corticosteroids; and the use of antimicrobial therapy in the expectant management of preterm rupture of membranes.
Current guidance suggests that preterm infants with sequential cranial ultrasound that do not show parenchymal haemorrhage, grade 3 or 4 intraventricular haemorrhage, cystic PVL or post haemorrhagic ventricular dilatation are unlikely to suffer from cerebral palsy. Therefore it is unlikely that conventional MRI will provide any significant additional diagnostic or prognostic information.
MRI should be considered however, if there is evidence of overt parenchymal injury on cranial ultrasound. An MRI may reveal abnormalities in the white matter, cerebellum and posterior limb of internal capsule that were previously unrecognised on cranial ultrasound scan and may be of prognostic significance.
MRI should be considered in babies with the following parenchymal abnormalities:-
- Cystic Periventricular Leucomalacia (PVL)
- Haemorrhagic parenchymal infarction (Grade 4 PVH)
- Moderate to severe post-haemorrhagic ventricular dilatation
- Echo densities persisting for more than 3-4weeks.
MRI may also be useful for preterm infants with unexplained abnormal neurological signs because of its increased sensitivity for detecting acquired lesions and CNS malformations.
The optimal timing for MR imaging of the preterm infant is 38-42 weeks corrected gestation as this allows for assessment of brain maturation and myelination in the posterior limb of the internal capsule. In exceptional circumstances an earlier MRI may be beneficial if the responsible consultant neonatologist considers it necessary to make an early diagnosis of neurological disease and appropriate facilities for imaging the preterm infant are available.
The final decision regarding any preterm infant undergoing an MRI scan should be made by the patient’s consultant. A discussion with the patient’s parents is important prior to the scan to explain the reasons for arranging an MRI and to also ensure that the parents understand that further follow up post MRI is required to fully assess their child’s neurodevelopment.
A recent audit performed in a tertiary neonatal unit within NHS GGC has shown that this would equate to approximately 9 extra MRI’s per year if the above criteria are used as guidance for performing an MRI.
Therefore an MRI should be ideally booked on or shortly after the discharge date of the baby to avoid the need for the neonatal transport service to become involved in the care of the patient. In addition this is the optimum time for the baby to undergo the MRI by the ‘feed and sleep’ method rather than undergoing a general anaesthetic. MRI under general anaesthetic should only be undertaken for diagnostic purposes or where interventions may be required, such as a possible VP shunt insertion for post haemorrhagic ventricular dilatation.
From: Phumza Nongena, Ash Ederies, Denis V Azzopardi, A David Edwards. Confidence in the prediction of neurodevelopmental outcome by cranial ultrasound and MRI in preterm infants. Arch Dis Child Fetal Neonatal Ed 2010;95:F388-F390.
Table 1
Prediction of abnormal neuromotor function by cranial ultrasound
|
Cerebral palsy |
|||
|
Ultrasound test result |
Pre-test probability |
Likelihood ratios (95% CI) |
Post test probability (95% CI) |
|
Normal scan |
9% |
0.5 (0.4 to 0.7) |
5% (4% to 6%) |
|
Grade 1 or 2 PVH |
9% |
1 (0.4 to 3) |
9% (4% to 22%) |
|
Grade 3 PVH |
9% |
4 (2 to 8) |
26% (13% to 45%) |
|
Grade 4 haemorrhage (any) |
9% |
11 (4 to 31) |
53% (29% to 76%) |
|
Cystic PVL |
9% |
29 (7 to 116) |
74% (42% to 92%) |
|
Ventricular dilatation |
9% |
3 (2 to 4) |
22% (17% to 28%) |
|
Hydrocephalus |
9% |
4 (1 to 13) |
27% (10% to 56%) |
Normal scan refers to absence of haemorrhage within the brain parenchyma or ventricles, cysts or ventricular dilation. The grade of PVH (intraventricular haemorrhage) is given according to the Papile classification. PVL indicates periventricular Leucomalacia. Ventricular dilation indicates moderate to severe ventricular dilation not meeting the criterion for hydrocephalus. Hydrocephalus indicates massive ventricular dilation >4 mm above the 97th centile. Pre-test probability refers to the prevalence of cerebral palsy based on the Epipage study.4 The likelihood ratio is the probability that a patient with cerebral palsy has a positive test (abnormal ultrasound result). Post-test probability is the probability that a patient with a specific abnormality on cranial ultrasound will have abnormal neuromotor function.
Westra S, Adler I, Batton D et al. Reader variability in the use of diagnostic terms to describe white matter lesions seen on cranial scans of severely premature infants: the ELGAN study. J Clin Ultrasound 2010;38(8):409-19
Davis PJ, Cox RM & Brooks J. Training in neonatal cranial ultrasound: a questionnaire survey. Br J Radiol 2005;78(295):55-6
Rennie JM. Neonatal cerebral ultrasound. Cambridge University Press (1997)
Kuban KCK, Allred EN, O’Shea TM et al. Cranial ultrasound lesions in the NICU predict cerebral palsy at age 2 years in children born at extremely low gestational age. J Child Neurol 2009;24(1):63-72
Berger R, Bender S, Sefkow S et al. Peri/intraventricular haemorrhage: a cranial ultrasound study on 5286 neonates. Eur J Obstet Gynecol Reprod Biol. 1997;75(2):191-203
Horsch S, Skiold B, Hallberg B et al. Cranial ultrasound and MRI at term age in extremely preterm infants. Arch Dis Child Fetal Neonatal Ed 2010;95(5):F310-4
Papile LA, Burstein J, Burstein R et al. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 1978;92(4):529-34
Harding D, Kuschel C & Evans N. Should preterm infants born after 29 weeks’ gestation be screened for intraventricular haemorrhage? J Paediatr Child Health 1998;34(1):57-9
Harris NJ, Palacio D, Ginzel A et al. Are routine cranial ultrasounds necessary in premature infants greater than 30 weeks gestation? Am J Perinatol 2007;24(1):17-21
Boal DK, Watterberg KL, Miles S et al. Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants. Pediatr Radiol 1995;25:425-28
Veyrac C, Couture A, Saguintaah M et al. Brain ultrasonography in the premature infant. Pediatr Radiol 2006;36:626-635
Technical Standard – Neonatal Cranial Ultrasound Scans by the British Society for Paediatric Radiology: http://www.bspr.org.uk/docs/Headfinal2.pdf
Beek E & Groenendaal F. Neonatal Brain US. The Radiology Assistant by The Radiological Society of the Netherlands: http://www.radiologyassistant.nl/en/440c93be7456f
Pourcelot L. Diagnostic ultrasound for vascular disease. In: Donald I, Levi S, editors. Present and future in diagnostic ultrasound. Rotterdan: Kooker; 1976 p141.
Dani C, Poggi C, Bertini G et al. Method of delivery and intraventricular haemorrhage in extremely preterm infants. J Matern Fetal Neonatal Med 2010;23(12):1419-23
Beaino G, Khoshnood B, Kaminski M et al. Predictors of cerebral palsy in very preterm infants: the EPIPAGE prospective population-based cohort study. Dev Med Child Neurol 2010;52(6):e119-25
Laskin MD, Kingdom J, Toi A. Perinatal and neurodevelopmental outcome with isolated fetal ventriculomegaly: a systematic review. J Matern Fetal Neonatal Med 2005;18(5):289-98
Bloom S, Bloom D, Dellanebbia C et al. The developmental outcome of children with antenatal mild isolated ventriculomegaly. Obstet Gynecol 1997;90(1):93-7
Nomura ML, Barini R, De Andrade KC et al. Congenital hydrocephalus: gestational and neonatal outcomes. Arch Gynecol Obstet 2010;282(6):607-11
Royal Prince Alfred Hospital Newborn Care Guidelines: http://www.sswahs.nsw.gov.au/rpa/neonatal/
An audit of 2 year developmental outcomes for infants with PVL. Dr Stewart Guthrie
Roberton NRC. Textbook of Neonatology. Churchill Livingstone (1992)
Crowther CA, Hiller JE, Doyle LW, Haslam RR; Australasian Collaborative Trial of Magnesium Sulphate (ACTOMg SO4) Collaborative Group. Effect of magnesium sulfate given for neuroprotection before preterm birth: a randomized controlled trial. JAMA. 2003 Nov 26;290(20):2669-76.
Northern Neonatal Nursing Initiative Trial Group. Randomised trial of prophylactic early fresh frozen plasma or gelatin or glucose in preterm babies. The Lancet 1996;348:229-232
Benson J, Drayton M, Hayward C et al. Multicentre trial of ethamsylate for prevention of periventricular haemorrhage in very low birthweight infants. The Lancet 1986;ii:1297-1300
Sinha S, Davies J, Toner N et al. Vitamin E supplementation reduces the frequency of periventricular haemorrhage in very preterm babies. The Lancet 1987;28:266-471
Fowlie PW. Prophylactic indomethacin: systemic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed; 1996 Mar;74(2):F81-7.
Elstad M, Whitelaw A, Thoresen M. Cerebral Resistance Index is less predictive in hypothermic encephalopathic newborns. Acta Paediatr. 2011 Oct;100(10):1344-9. doi: 10.1111/j.1651-2227.2011.02327.x. Epub 2011 May 18.
Brouwer A, Groenendaal F, van Haastert IL. . Neurodevelopmental outcome of preterm infants with severe intraventricular hemorrhage and therapy for post-hemorrhagic ventricular dilatation. J Pediatr 2008;152:648–54.
Phumza Nongena, Ash Ederies, Denis V Azzopardi, A David Edwards. Confidence in the prediction of neurodevelopmental outcome by cranial ultrasound and MRI in preterm infants Arch Dis Child Fetal Neonatal Ed 2010;95:F388-F390 doi:10.1136/adc.2009.168997
British Association of Perinatal Medicine; Fetal and Neonatal Brain Magnetic Resonance Imaging: Clinical Indications, Acquisitions and Reporting; February 2016; Available URL: https://www.bapm.org/publications/documents/guidelines/BAPM%20MRI%20standards%20for%20fetal%20neonatal%20brain%20imaging_FINAL%20SUBMISSION%20080216.pdf
An audit reviewing diagnosis of brain injury on CrUSS – Dr Andrew Brunton
Last reviewed: 08 May 2018
Next review: 30 April 2023
Author(s): Dr. Martina Rodie – SpR Paediatrics & Dr Andrew Powls – Neonatal Consultant PRM. Update (September 2017) by Dr. Andrew Brunton – ST7 Neonatal GRID Trainee
Co-Author(s): Other Professionals Consulted: Dr. Anne Marie Heuchan – Neonatal consultant RHSC, Dr. Andrew Watt – Radiology Consultant RHSC
Approved By: West of Scotland Neonatal Managed Clinical Network