

 GGC Paediatric Guidelines
GGC Paediatric Guidelines


|
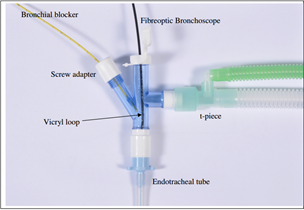
Assemble these items before connection to the patient. Screw adaptor should be opened enough to allow easy movement of blocker. |
LUBRICATE WELL - it's easy to damage the small scope |
|---|

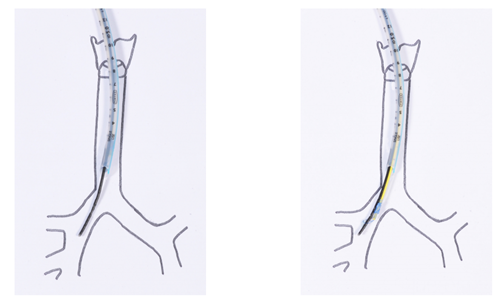
Advance the scope into the bronchus, then advance the blocker over the bronchoscope.
You may need the vicryl loop a bit tighter than shown on the above picture.

Withdraw the bronchoscope but keep the balloon on the blocker in view, inflate the balloon under direct vision until it just occludes the bronchus & note the volume required.
When the blocker is confirmed as in the correct position, tighten the screw adapter to keep it secure & remove the vicryl loop by unscrewing the red & white cap from the proximal end of the blocker.



