
Pre-operative management of anticoagulation therapy pathway for paediatric patients with congenital heart disease
exp date isn't null, but text field is
Objectives
To provide a consistent and safe approach to the preoperative management of anticoagulation therapy for paediatric patients with congenital heart disease (CHD)
Scope
Applies to all pre-operative paediatric patients with congenital heart disease receiving anticoagulation therapy.
Audience
All health care professionals providing pre-operative care to paediatric patients with congenital heart disease receiving anticoagulation therapy should be familiar with this guideline
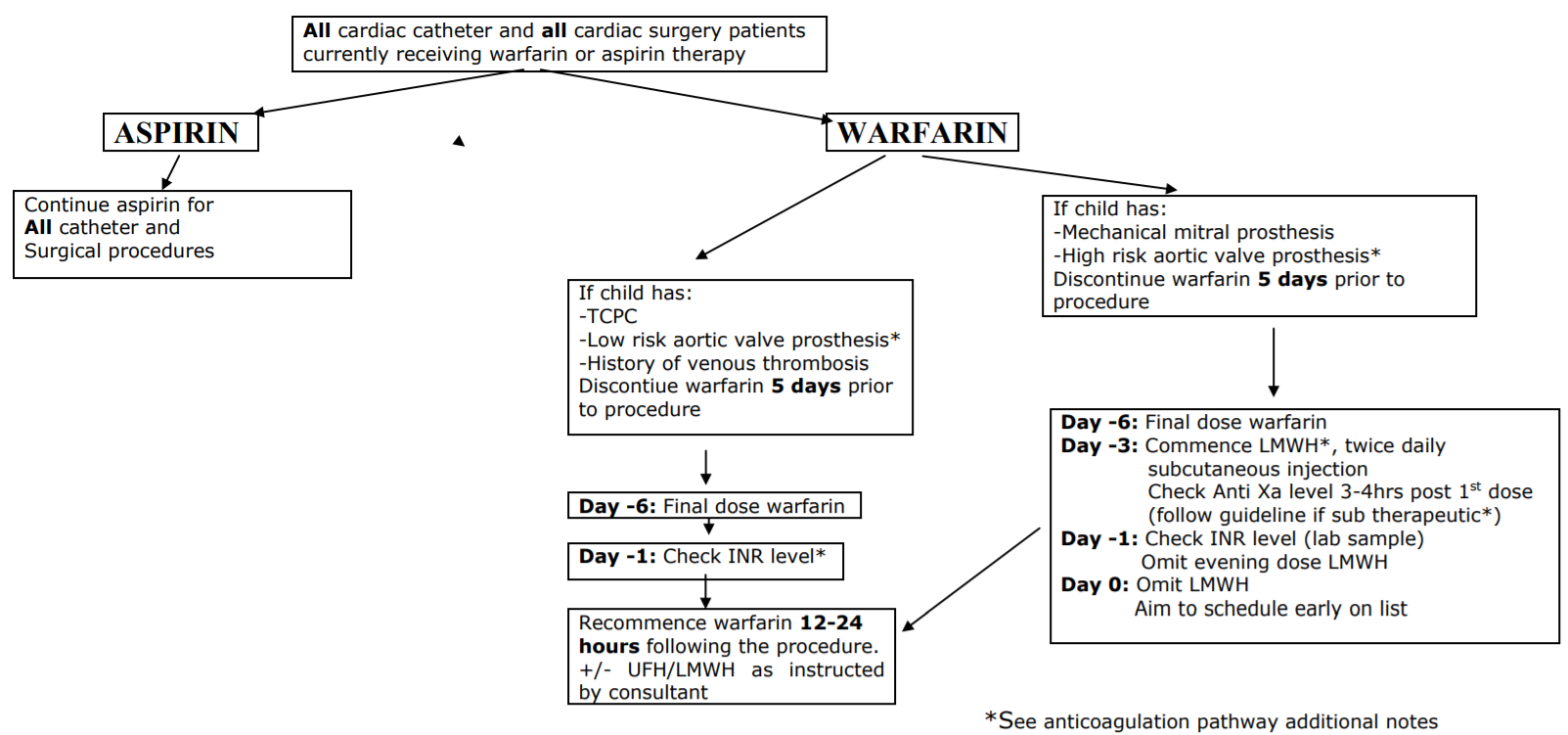
Aortic Valve Prosthesis
Low Risk
A standard bi-leaflet aortic valve prosthesis with no additional risk is considered low risk.
High Risk
An increased risk of thrombosis may result from a number of factors, including:
- Previous thromboembolism
- Left ventricular dysfunction
- Hypercoagulable conditions
- Atrial fibrillation
Therapeutic low molecular weight heparin (Enoxaparin) should be administered for these situations as per the pathway for mechanical mitral valve prosthesis.
Low Molecular Weight Heparin (LMWH) For bridging to cardiac catheter/surgery
Dosing
| <2 months of age >2 months of age |
1.5mg/kg twice daily 1mg/kg twice daily |
Anti Xa level
3-4 hours post dose
Order ‘control of heparin – child’ on trakcare
Target range 0.5-1 i.u/ml
Guideline for adjusting dose: Anticoagulation Therapy for Post Op Cardiac Patients in PICU
If level sub therapeutic (low) adjust dose, re prescribe enoxaparin for current time and 12 hourly thereafter (do not wait until next dose is due).
Administration
Do not administer Enoxaparin via insuflon.
Doses of <0.1ml in volume to be diluted up to 0.1ml with 0.9% sodium chloride
INR Level
If INR is >2 when checked on day -1, inform the consultant cardiac anaesthetist and the cardiology consultant on call, so a decision for reversal can be made.
If reversal is appropriate:
- Seek haematology advice
- As per BNF for Children: Vitamin K 30micrograms/kg IV or oral (max 1mg) If given orally, use Konakion MM Paediatric
Dental surgery in children receiving warfarin therapy
Follow: Anti Thrombotic Protocol
Baglin TP & Rose R E. (1998) Guidelines on oral anticoagulation, 3rd edition, British Journal of Haematology, vol 101, pp 374-387
British National Formulary for Children
Begg C. (2015) Anticoagulation Therapy for Post Op Cardiac Patients in PICU: NHSGGC
Chalmers E. (2014) Anti-thrombotic Protocol: NHSGGC
Chan A, David M, Massicotte P. (2009) Cincinnati Children’s Hospital Medical Center Best Evidence Statement Management of warfarin therapy
Douketis, J.D. (2011) Perioperative management of patients who are receiving Warfarin therapy: an evidence-based and practical approach. Blood. Vol 17, no 19, pp 5044-5049
Hirsh J, Guyatt G, Albers G, Harrington R & Schunemann H. (2008) Executive summary : American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 8th Edition, Chest, vol 133, 71S-10S
Motz,R., Wessel,A., Ruschewski,W. & Bursch,J. (1999) Reduced frequency of occlusion of aorto-pulmonary shunts in infants receiving aspirin. Cardiol. Young. 9, 474-477
Palaniswamy C, Selvaraj DR (2011) Periprocedural bridging anticoagulation : current perspectives. American Journal of Therapeutics. Vol 18 pp 89-94
Tweddell,J.S. (2007) Aspirin: a treatment for the headache of shunt dependent pulmonary blood flow and parallel circulation? Circulation 116, 236-237
Last reviewed: 23 July 2020
Next review: 23 July 2023
Author(s): Alison Buller
Version: 2
Approved By: Paediatric & Neonatal Clinical Risk & Effectiveness Committee