Patient identification in Outpatients
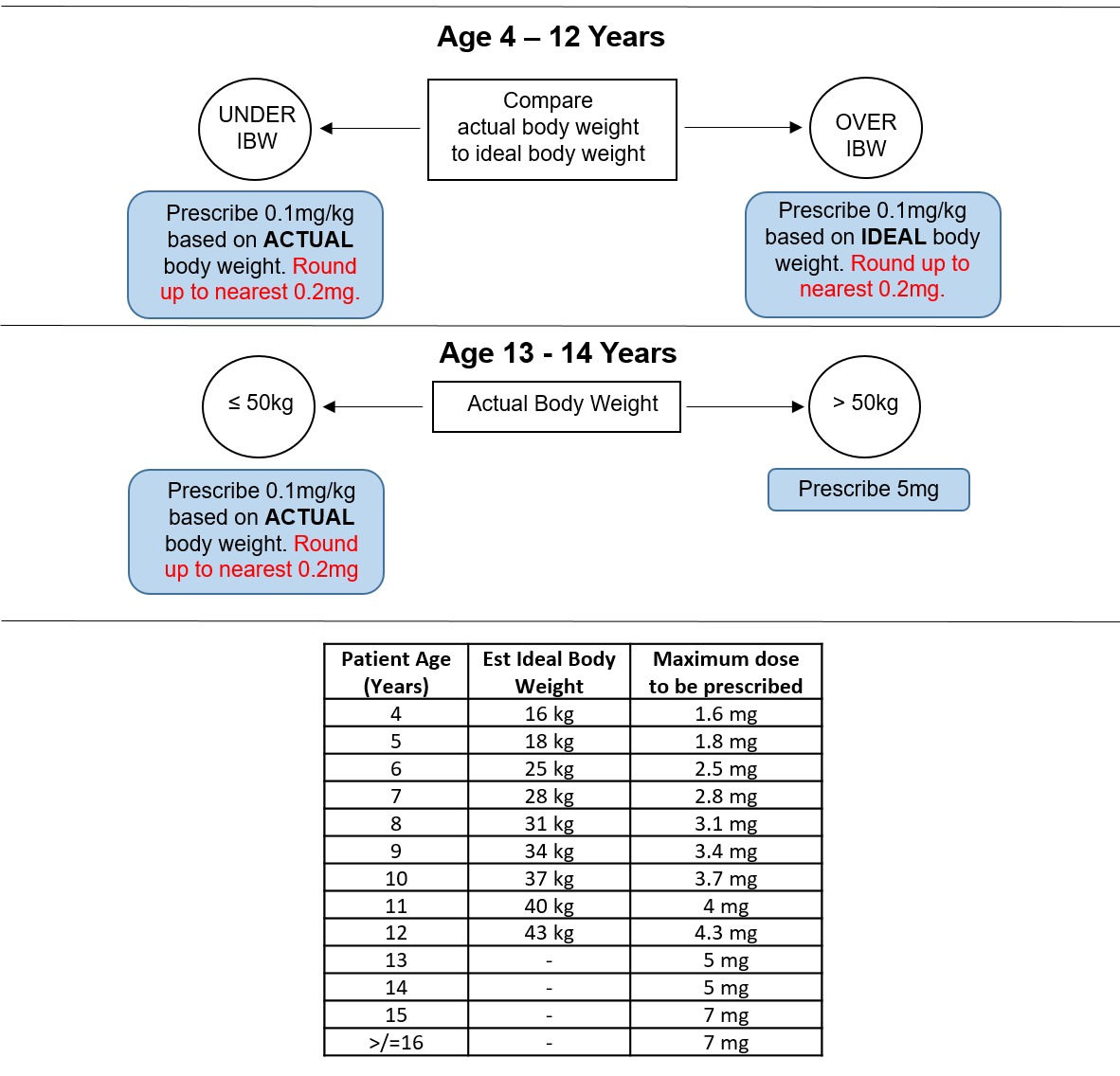
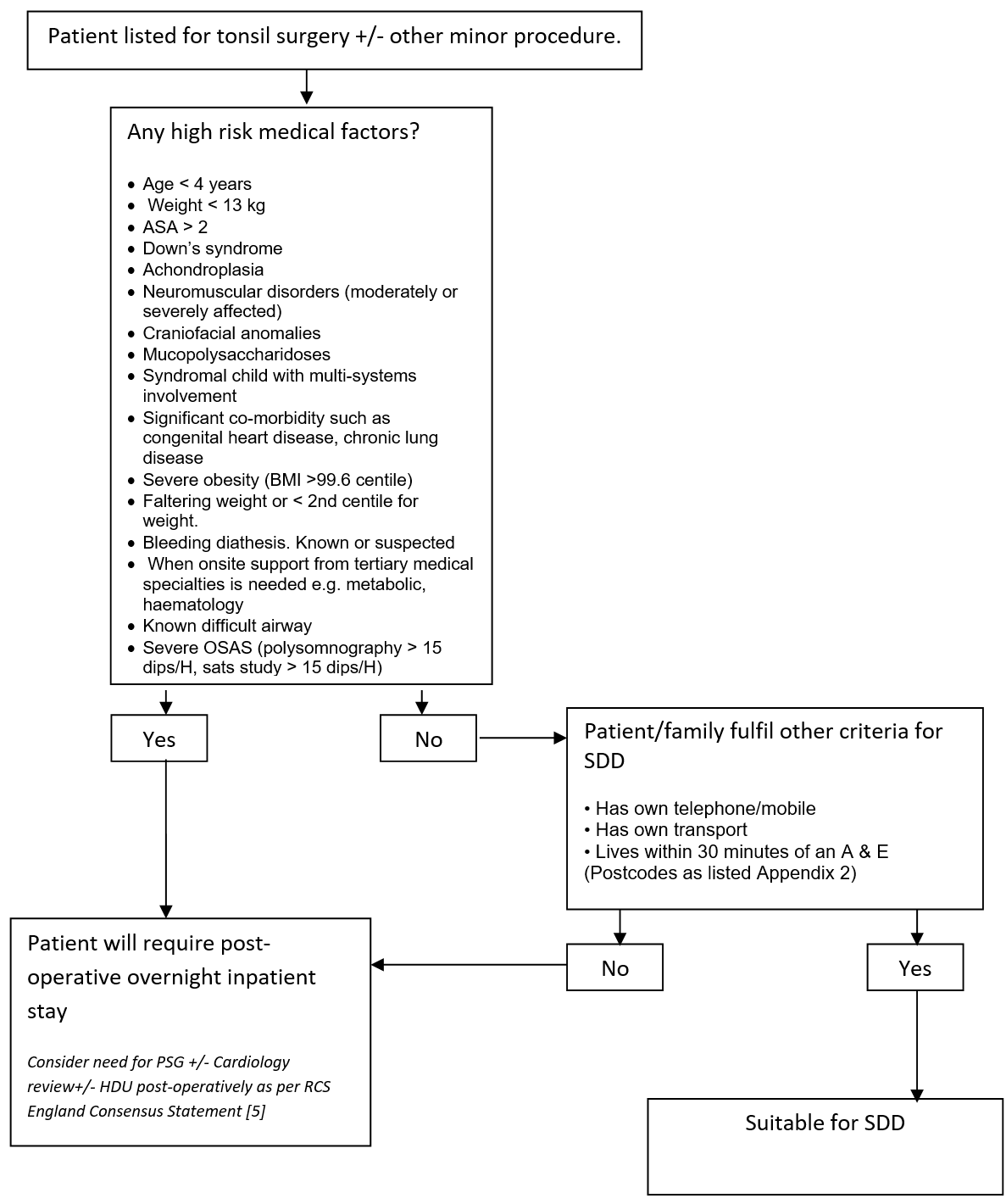
Patients listed for tonsil surgery with or without any other minor procedure at time of initial consultation will be assessed by the listing surgeon or nurse specialist as to appropriateness on a medical basis for SDD. Absolute exclusion criteria are listed in Appendix 1. Surgeons will discuss the possibility of SDD with patient and family at the time of consultation. If agreed then the listing clinician will either in the “Remarks” box “suitable for SDD” or “SDD” or in the length of stay mark this as “0”. Sleep studies (overnight saturation monitoring or polysomnography) for children listed for this surgery will be undertaken as per the recommendations in the “Tonsillectomy and adenoidectomy in children with sleep-related breathing disorders: consensus statement of a UK multidisciplinary working party” [5] and are otherwise not routinely required, unless at the discretion of the listing surgeon, or as per the recommendation of the “Safe Delivery of Paediatric ENT Surgery In The UK: A national Strategy. A combined Working Party of the British Association for paediatric Otolaryngology (BAPO), ENT UK, The Royal College of Anaesthetists (RCoA) and the Association of the Paediatric Anaesthetists of Great Britain and Ireland” [4].
Pre-assessment Clinic
The Pre-assessment Nurses will assess the patient within two weeks of surgery. They will check/confirm that the listing clinician has listed the child for SDD. They will confirm that no significant changes have occurred in the child’s general medical status. They will re-assess for appropriateness of SDD including medical and social factors as described in this document.
Social factor questions are listed in Appendix 1. Postcode look up in Appendix 2.
Where a child who was previously identified as being a potential candidate for SDD is felt to be ineligible they will inform the family and contact the ENT Secretaries to alert them to this.
Where appropriate the Pre-assessment Nurses will counsel children and their families regarding the SDD protocol.
The Pre-assessment Nurses will also counsel families to obtain their first line post-operative analgesia (paracetamol and ibuprofen) from a Pharmacy First Pharmacy. They will also counsel that their child's surgery may be undertaken on a same day discharge basis.
When seeing children face to face a weight will be obtained and uploaded to iGrow.
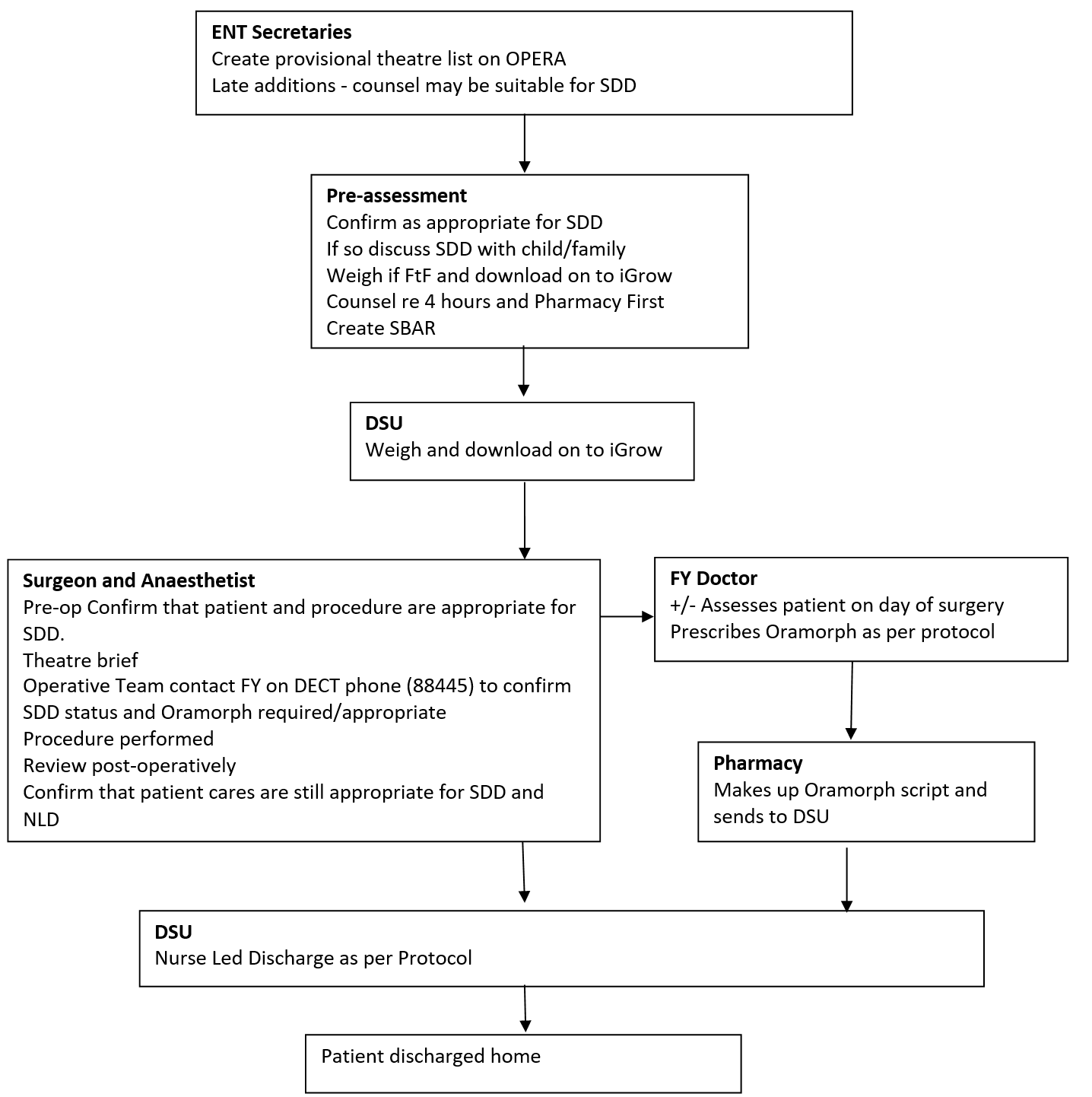
The Pre-assessment team will email an SBAR to DSU ward the night before surgery. The SBAR will include which tonsil patients are appropriate to have their surgery undertaken as SDD surgery patients.
ENT Secretaries
At present up to 20% of children will not be able to be pre-assessed (personal communication), due to short notice changes and other variables. If the listing clinician has identified a patient, who it was felt could have their surgery performed as a SDD procedure and who has not attended/been able to be assessed by the Pre-assessment Team, the Secretary will contact the family to check availability and to let them know their date of surgery. The Secretary will ask the social factors as stated in Appendix 1 to assess appropriateness for SDD, and inform the family regarding the possibility of SDD. The Secretaries will then construct the Theatre list to accommodate this using this and the information obtained from the Pre-assessment Team.
Postcode criteria will be used to identify patients suitable for SDD. These postcodes must be within a 30 minute drive of an A & E in the Greater Glasgow and Clyde and Lanarkshire NHS Trusts. (included are all G postcodes except G63, G82-4, PA postcodes PA 1-19, ML postcodes ML1-11).


 GGC Paediatric Guidelines
GGC Paediatric Guidelines