GGC Paediatric Guidelines
GGC Paediatric Guidelines

- The Hamilton T1 can ventilate ALL patient sizes (neonate-adult) and can give a continuously adjustable FiO2 from 21 – 100% (unlike some other transport ventilators which allow only fixed options (e.g. air/60%/100%)
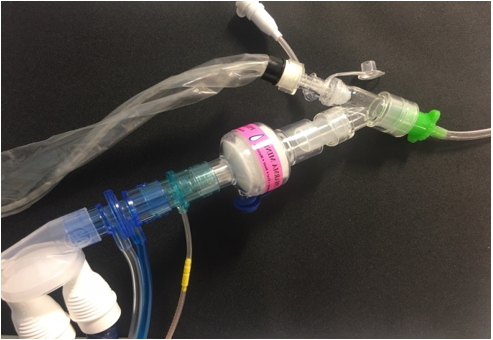
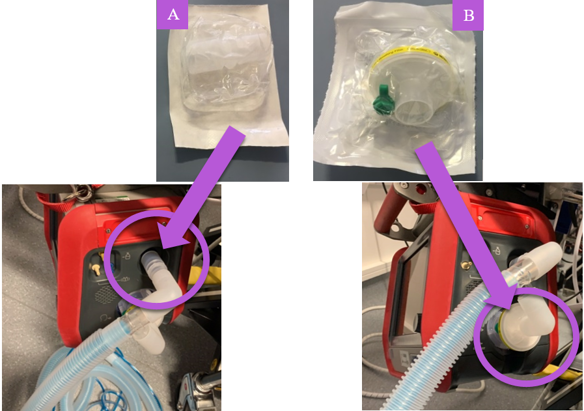
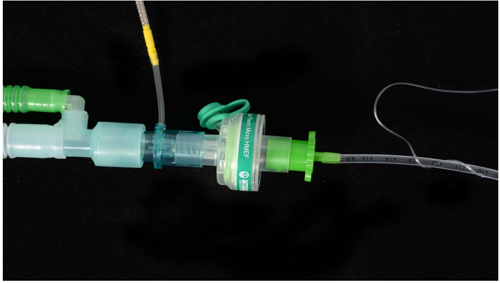
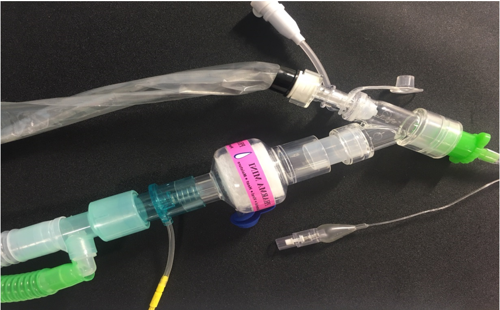
- It has TWO different breathing circuit types depending on patient size
- It has TWO different expiratory valve types depending on patient size
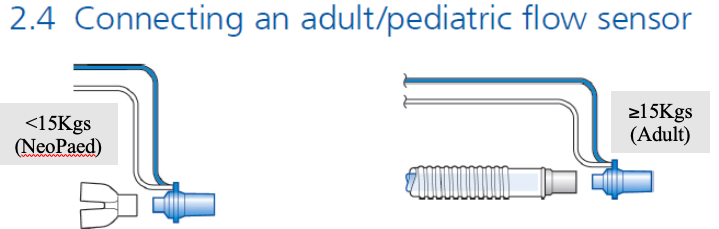
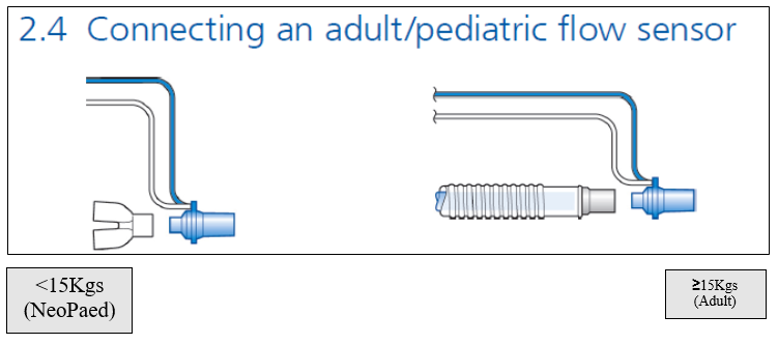
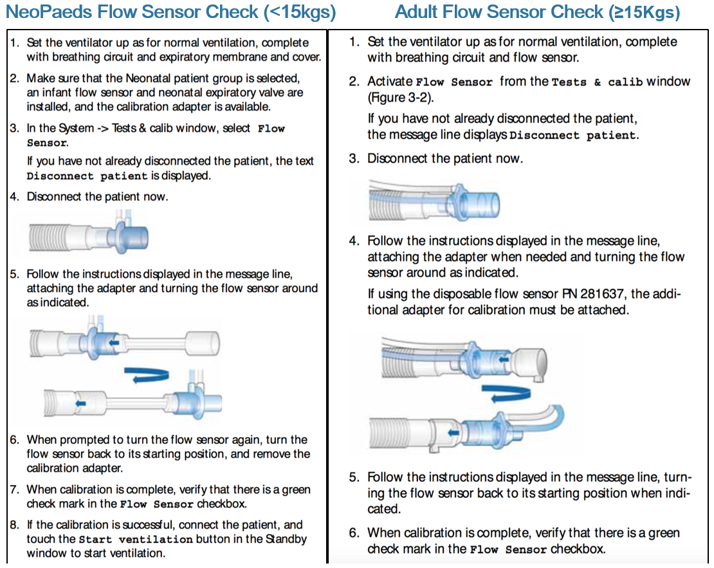
- It has TWO different flow sensor types depending on patient size
- TABLE 1 summarises the different potential configurations of these
- It does NOT deliver heated-humidified gas without the addition of a passive or active humidfication device. Ventilation without humidification presents a risk of airway obstruction from retained secretions and also increases insensible water loss. It is to be AVOIDED.
- It can deliver Non-Invasive Ventilation (NIV), HiFlo as well as invasive ventilation modes. We will not be using it for mobile HiFlo.
- It has TWO internal batteries and a mains plug. It should remain PLUGGED IN when not in use or when static,
- Power consumption is VARIABLE depending on settings
- A transfer should not be commenced if the battery icon is reading below 70%
- It uses 4-bar Medical Oxygen via a Schrader valve. Oxugen cylinder heads used in RHC may have either a TWIST RELEASE or PUSH RING RELEASE Schrader valve to disconnect the ventilator from the cylinder head.
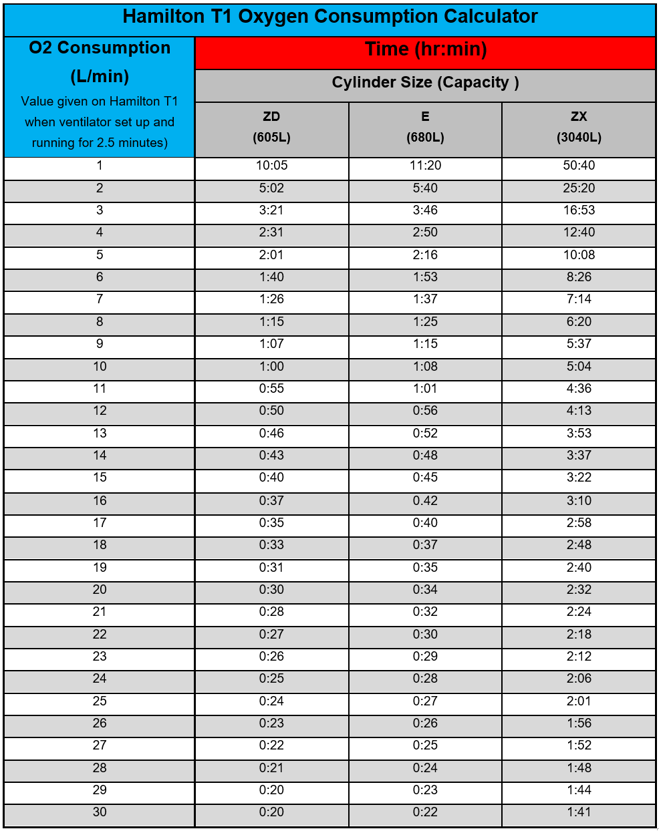
- Oxygen consumption is VARIABLE depending on settings
- see TABLE 2 for more details
- for
- It is not MRI compatible.
- Patient monitoring during transfer will be delivered by standard PICU Philips X3 transport monitors or equivalent (i.e. in RHC we do NOT use the Hamilton T1’s internal ability to monitor SpO2 & etCO2..
WHERE TO FIND IT
- The Hamilton T1 is stored on the bench on the right side of the PICU Clean Utility Room at Staff Base 2.
If the machine is still in use on another patient, a loan T1 can be obtained from the four machines in ED Resus at the discretion of the ED Charge Nurse.
(Remember to CLEAN IT and RETURN to ED after use.) - It should ALWAYS be plugged into mains power when not in use