
High Frequency Oscillatory Ventilation (HFOV) : a guide to the use of HFOV in the neonate
exp date isn't null, but text field is
Objectives
This document is a guide to the theory and practical techniques for the use of High Frequency Oscillatory ventilation (HFOV) in the neonate. This mode of ventilation may be useful in settings where conventional modes are failing to achieve adequate ventilation or may result in significant pulmonary injury, or where HFOV is considered to be better suited to underlying lung pathophysiology. The decision to use HFOV is individualized and must be made by experienced senior clinicians.
High frequency oscillatory ventilation (HFOV) utilises rapid ventilation rates with small tidal volumes (often less than anatomical dead space) and active inspiratory AND expiratory phases. A constant distending airway pressure is applied to the alveoli which aims to maximise functional residual capacity and ventilation/perfusion matching, over which small tidal volumes are superimposed at a high rate.
The aim of using HFOV is to reduce ventilator associated lung injury when high airway pressures and volumes in conventional ventilation modes are required to maintain adequate gas exchange. When initiated early, high frequency oscillatory ventilation may improve oxygenation and reduce risk of lung injury in neonates and infants.
2.3 Adjusting the MAP for optimal lung recruitment – “Recruitment Manoeuvre”
2.7 Making Adjustments Once Established on HFOV
2.10 Potential Complications – HFOV
HFOV may be used as an alternative to conventional ventilation in a number of disease settings. HFOV may be reserved as a “rescue therapy” when adequate oxygenation and/or ventilation cannot be achieved on CMV. Alternatively, HFOV may be employed to minimise lung injury by avoiding use of high inspiratory pressures or FiO2 on CMV.
Particular disease settings where HFOV may be appropriate include lung disease in:
- Neonatal Respiratory Distress Syndrome (RDS)
- Chronic lung disease of prematurity
- Meconium Aspiration Syndrome (MAS)
- Congenital Diaphragmatic Hernia (CDH)
- Neonatal Air-leak Syndrome with pulmonary interstitial emphysema
- Pneumonia
- Pulmonary Haemorrhage
- Hypoplastic lungs
Please discuss the decision to commence HFOV with the attending consultant.
Pre-Checks:
- Ensure blood pressure and intravascular volume is adequate before transferring to HFOV, as blood pressure may fall rapidly, especially in babies with perfusion problems in Sepsis / NEC. Consider volume expansion to avoid a sharp fall in cardiac output. If BP not improving after volume expansion, consider starting inotropic support.
- Consider invasive BP monitoring if possible.
- Correct metabolic acidosis.
- ETT leak - Consider upsizing ET tube
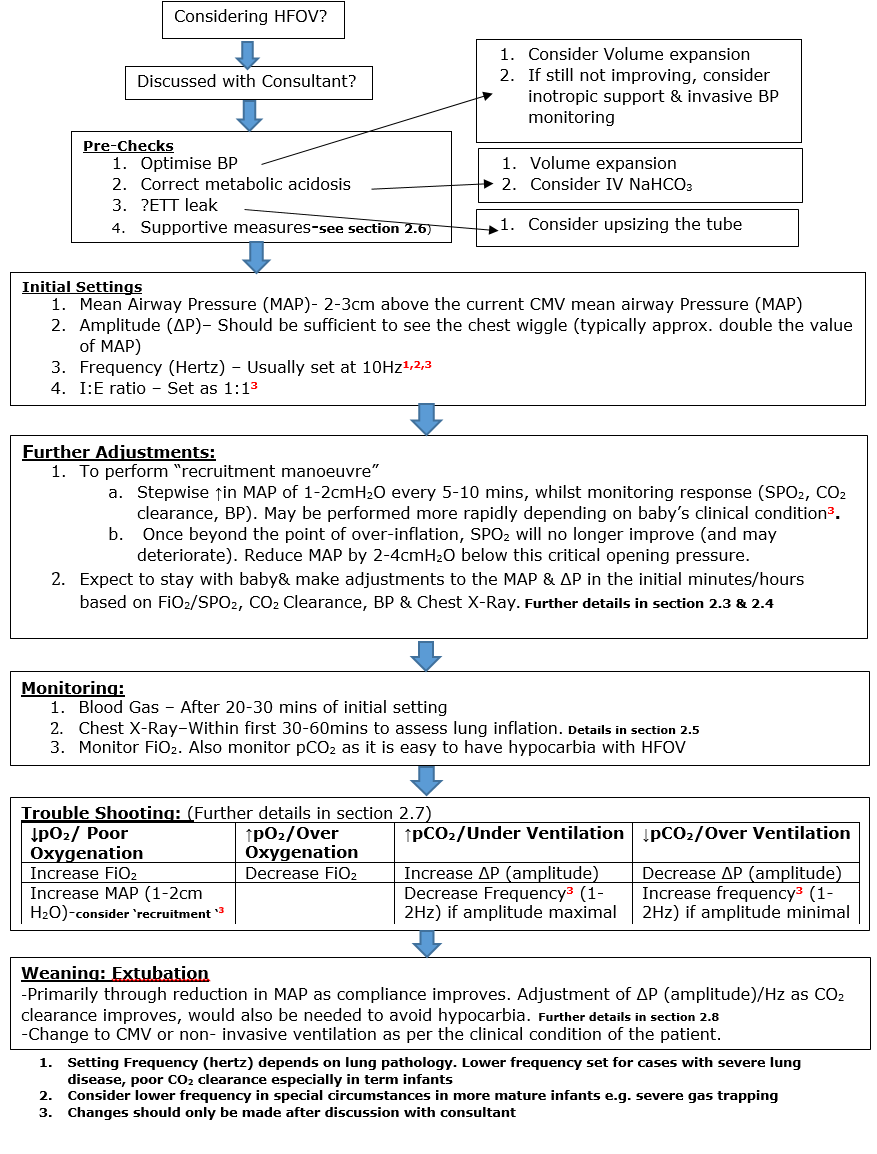
Initial settings:
Initial settings will be prescribed by medical staff, however the following is a guide:
- Mean Airway Pressure (MAP): Generally the starting MAP is set 2-3cm above the current CMV mean airway pressure. However, to achieve optimal lung recruitment the operator should be prepared to start a recruitment manoeuvre – see section 2.3.
- Typical operating range for MAP will be between 10 to 16 cmH2O. If Higher MAPs are required, for example in in severe lung disease with very poorly compliant lungs, then they should be used with caution and careful monitoring to avoid over distension and air leak. In situations of severe gas trapping, or air leak, a lower MAP may be selected
- Amplitude (ΔP): Set the amplitude (ΔP) to approximately double the value of the MAP, sufficient to see a chest “wiggle” from the level of the nipple to the umbilicus. The starting amplitude required to achieve adequate “wiggle”, may in due course be reduced after initial lung recruitment, to avoid hypocarbia.
- Typical operating ranges for ΔP (amplitude) will between 20 to 30Hz. Higher ΔP (amplitude) should only be used with caution only in severe lung disease.
- Frequency/Hertz: Set appropriate frequency / hertz (determined by lung pathology and clinical condition): Usually frequency is set at 10 Hz. Lower frequencies may be used in severe lung disease, with poor CO2 clearance, especially in term infants.
- I:E Ratio: I:E ratio is usually 1:1 and not changed except in special circumstances (e.g. severe gas trapping).
Other considerations
- Set appropriate FiO2 and titrate according to patient response and desired oxygen saturation range.
- Obtain a blood gas within 20-30 minutes and adjust settings as appropriate.
- Obtain a chest x-ray after commencing HFOV to determine lung expansion, ideally within one hour. X-ray should show around 8 rib spaces
Expect to stay with the baby and make adjustments to the MAP and ΔP (amplitude) in the first minutes of the initial hour of starting HFOV, based on oxygenation, CO2 clearance, hemodynamic (BP) and chest x-ray.
2.3 Adjusting the MAP for optimal lung recruitment – “Recruitment Manoeuvre”
On commencement of HFOV it is useful to ensure that optimal lung volume has been achieved (as discussed earlier). MAP is used to achieve and maintain the maximal recruitment of alveoli. Both under-inflation and over-inflation of the lungs will give sub optimal oxygenation.
- Practically, this may involve a “recruitment manoeuvre”: i.e. a stepwise increase in MAP of 1-2cmH2O whilst monitoring response (oxygenation, CO2 clearance, BP). Usually the MAP would be incremented every 5-10 minutes, but more rapid increments in MAP, every 1-2 minutes, might be required depending on the clinical condition, (for example, in a baby with severe oxygenation problem with a collapsed lung volume).
- Beyond the point of over-inflation (critical opening pressure) oxygenation will no longer improve (and may deteriorate). MAP should then be reduced back to 2-4cmH2O below this critical opening pressure. You have now performed a “recruitment manoeuvre” and for the same MAP have achieved a greater lung volume and improved gas exchange.
- Recheck a blood gas 20 minutes after making a change. It is easy to cause hypocarbia with HFOV. MAP has very little effect in CO2 clearance in an infant with adequate lung inflation, but may cause rapid drops in PaCO2 during lung recruitment. (NB – such rapid falls in CO2 may be predicted by a significant rise in the tidal volume measurement (VThf). This parameter is usefully monitored during the recruitment process – see section 2.4)
- Typical operating range for MAP will be between 10 to 16 If Higher MAPs are required, for example in in severe lung disease with very poorly compliant lungs, then they should be used with caution and careful monitoring to avoid over distension and air leak.
Ventilation (CO2 clearance) in HFOV is controlled by the DP (amplitude), for a given level of lung inflation. It is also influenced by the frequency of oscillation (Hz). Decreasing the frequency can cause markedly increased CO2 elimination and should not be done without discussion with the attending consultant.
In response to pCO2 measurements adjust the DP (amplitude) in increments of 2-4.:
- Increase ΔP (amplitude) in response to a raised pCO2
- Reduce ΔP (amplitude) in response to a low pCO2
Typical operating ranges for ΔP (amplitude) will be between 20 to 30cm H2O. Higher ΔP (amplitude) should only be used with caution only in severe lung disease.
Always observe the chest wall to make sure that it is still vibrating. Recheck a blood gas 20 minutes after making a change.
Ventilation parameter during HFOV
End tidal CO2 monitoring does not work during HFOV and other trends in ventilatory parameters should be monitored and charted.
- Tidal volume (VThf): VThf is typically around 2ml/kg although monitoring trends rather than absolute value may be more meaningful.
VThf is strongly influenced by the internal diameter of the tracheal tube. When HFOV is used without volume guarantee, halving the tracheal tube internal diameter (e.g., due to secretions) will increase the resistance by 16 fold, and markedly reduce tidal volume. Small increases in resistance are also evident with longer tracheal tubes. VThf is also influenced by the ΔP (amplitude), frequency and I:E ratio set for the patient.
(NB – When HFOV is used with VG, ventilators, which will make modifications to the DP to try to maintain tidal volume; however evidence is still evolving and being studied in neonates at this time. See section 3.8 for more details
- DCO2 (Gas transport co-efficient): This is derived using the tidal volume and frequency (DCO2 = frequency x (tidal volume)2. It varies for every baby depending on weight, disease and oscillatory frequency of HFOV. DCO2 requirements are lower, if the baby is breathing spontaneously and contributing to its own ventilation. As with VThf, higher values of DCO2 are associated with better CO2 clearance, but this should be used to monitor trends rather than to target a specific value. Also, baby’s clinical condition and other parameters should also be taken into account. Following table provides a guide to the expected DCO2 (mL2/kg2/s) required for babies at any given weight.
|
Weight (kg) |
0.5 |
1.0 |
2.0 |
3.0 |
|
DCO2 (mL2/kg2/s) |
10 |
40 |
160 |
360 |
There is no gold standard clinical test of lung volume. CXR can assist in assessing lung inflation. Obtain a CXR within the first 30 minutes of commencing HFOV and consider repeating within the first 12 hours. Thereafter, consider repeating CXRs with acute changes in the baby’s condition. Frequent CXR may be needed whilst establishing recruitment but may be able to be done less frequently once stable or cautiously weaning
The CXR should confirm the diaphragm to be lying between the 8th and 9th posterior ribs for optimal lung inflation.
Overinflation is indicated by:
- Diaphragm at 10+ ribs
- Intercostal bulging of the lungs
- Flattened diaphragm
- Thin cardiac silhouette
Underinflation is indicated by:
- Lung fields with areas of collapse / consolidation
- Lung fields expanded to less than the 6th rib posteriorly
- High diaphragm
In specific situations such as non-uniform lung disease with one side of the lungs collapsed, you might have to tolerate slight over distension in the good lung to encourage recruitment in the other side.
Ensure that related aspects of care are optimised, including:
- Sedation with an opiate (usually morphine) +/- muscle relaxation
(not routinely needed, but may be important in severe lung disease) - Positioning of baby’s neck – ensure a neutral position
- ETT Leak – consider upsizing if necessary
- ETT secretions/ obstruction – regular suction
- Positioning – Prone positioning, or side lying, improves oxygenation and tidal volumes of preterm infants with RDS
Lung volume loss during ETT disconnection e.g. suctioning:
If HFOV is briefly interrupted (e.g. due to ventilator disconnection, ETT suction) then there may be a loss of lung volume due to the drop in MAP. A recruitment manoeuvre may be required at this time to restore lung volume and optimise oxygenation and ventilation. Use of in-line suction, where available, can also prevent this.
2.7 Making Adjustments Once Established on HFOV:
|
↓PO2/ Poor Oxygenation |
↑ PO2/Over Oxygenation |
↑PCO2/Under Ventilation |
↓PCO2/Over Ventilation |
|
Increase FiO2 |
Decrease FiO2 |
Increase ΔP (amplitude) |
Decrease ΔP (amplitude) |
|
Increase MAP* |
|
Decrease Frequency** (1-2Hz) if amplitude maximal |
Increase frequency** (1-2Hz) if amplitude minimal |
*Consider recruitment manoeuvres – discuss with consultant
**Changes in frequency should only be made after discussion with consultant
Trouble Shooting During HFOV:
Low PO2: Consider:
- ET tube patency and position – Check for chest movement/wiggle & breath sounds, consider suction, could use Pedi-cap while giving manual breaths with neo-puff to check if ETT is in the airway
- Condensation/ rain-out in the ventilator circuit- slight elevation of the oscillation to assist with rain-out and enable good drainage
- Air leak/ Pneumothorax- Transilluminate, Urgent CXR, drain if needed
- Sub-optimal lung recruitment- Increment MAP or recruitment manoeuver, consider CXR
- Over inflated lung – Check BP, reduce MAP; does oxygenation improve, Consider CXR
High PCO2: Consider:
- ET tube patency and position – (as above)
- Under-inflated lungs, insufficient alveolar ventilation – Increase ΔP (amplitude) and look for improvement in chest wall movement, could decrease frequency(Hz) after discussion with consultant
- The disadvantage of high MAP is “Over inflation of lungs” which leads to decreased cardiac output and reduced BP, high pulmonary vascular resistance, decreased venous return and pulmonary leaks. It can lead to poor oxygenation and tissue perfusion, eventually leading to high CO2 levels in blood. It should be timely identified by means of clinical assessment, BP and CXR and corrected by reducing the MAP.
Weaning is primarily through reduction in the MAP as compliance improves, however it may also be necessary to adjust DP +/- frequency (Hz), as CO2 clearance improves, to avoid hypocarbia.
- It is important to maintain the lung volume during weaning. Reduce FiO2 as tolerated, and once less than around 30% begin weaning the MAP in increments of 1-2 cm H2O (except when over-inflation is evident).
- In air leak syndromes ,reducing MAP may take priority over weaning the FiO2
- Reduce ΔP (amplitude) in increments of 2-4, according to the paCO2. Remember to observe the chest wall to confirm vibration.
- If an acceptable paCO2 cannot be maintained by adjusting the DP (amplitude) alone then adjustments to the frequency (Hz) may be required. Changes in frequency should be discussed with the consultant.
- Deterioration in oxygenation may be due to either a MAP which is too low (atelectasis), or too high (over distension during the baby’s recovery phase). A CXR may help to distinguish these.
- Patients may be extubated from HFOV e.g. to Vapotherm or CPAP. Alternatively patients may be transitioned to conventional ventilation prior to extubation. When changing to conventional ventilation set an appropriate PEEP and then choose a PIP to give a MAP 1 - 2 cm H2O below the HFOV setting.
- Remember to wean sedation and start caffeine citrate, if indicated, in advance of extubation.
- Severe gas trapping/ cystic lung disease
- Lower frequency (6-8Hz) may assist in minimising gas trapping (possibly by allowing longer expiratory phases), and in turn improve oxygenation.
- Changing I:E ratio to 1:2 (normally 1:1) will prolong expiratory phase to minimise gas trapping.
- Air leak syndromes
A lower MAP many minimise air leak.
2.10 Potential Complications – HFOV
- Decreased cardiac output (therefore decreased mean blood pressure) associated with high mean airway and intra-thoracic pressure. Increased intra-thoracic pressure compresses the major vessels returning blood to the heart, it also acts to increase pulmonary vascular resistance thereby reducing pulmonary venous return to the left side of the heart and cardiac output to the systemic circulation.
Decreased cardiac output is a particular risk when initiating HFOV in an infant where central venous pressure may already be low e.g sepsis, NEC, low intravascular volume. Such patients may require volume expansion prior to commencing HFOV - Over-distension leading to pulmonary air-leaks
- IVH due to changes in cerebral circulation related to treatment with the oscillator.
3.4 Conventional ventilation vs HFOV: Fundamental Differences
3.5 Mechanism of Gas Transport in HFOV
3.6 Determinants of gas exchange in HFOV
3.7 Optimal Ventilation Strategy
3.8 HFOV with Volume Guarantee (HFOV-VG)
- To achieve and maintain optimal lung inflation
- To use the lowest Fi02
- To ensure optimal gas exchange while minimising the risk of ventilator induced lung injury
Mean Airway Pressure - a continuous distending pressure measured in cm H20
Amplitude/D P - the peak to trough measure of the pressure waveform. This is the measure of pressure the ventilator uses to push air into the circuit. ΔP (amplitude) creates the wiggle seen in HFOV.
Frequency - the rate at which oscillations are delivered. Expressed in hertz where 1 hertz = 60 breaths per minute
Functional Residual Capacity - the volume of air present in the lungs at the end of expiration
Dead Space - the air in the nose, mouth, larynx, trachea, bronchi and bronchioles where air does not come into contact with the alveoli of the lungs i.e. the portion of tidal volume that does not take part in gas exchange
Theories of of ventilator induced lung injury:
Volutrauma
The use of large tidal volumes to achieve adequate ventilation damages the pulmonary capillary endothelium, alveolar and airway epithelium. This mechanical damage causes fluid, protein, and blood to leak into the airways, alveoli and interstitial tissue of the lung and leads to progressive respiratory failure.
Atelectotrauma
Refers to the damage caused to a lung unit by repetitive opening and closing of the alveoli. This opening, collapse and reopening of alveoli causes surface forces which have the potential to damage the surface epithelium of the airways.
Barotrauma
Mechanical damage caused to the airways by the application of high positive airway pressures
Oxygen toxicity
The administration of excessive levels of oxygen and the action of oxygen free radicals is implicated in lung disease and in the development of retinopathy of prematurity. Un-scavenged oxygen free radicals have a direct effect on pulmonary epithelial cells leading to cell membrane injury. The lungs, in response to this damage tries to regenerate but the repair is fibrotic, which is typical of chronic lung disease in premature infants.
3.4 Conventional ventilation vs HFOV: Fundamental Differences
HFOV involves applying a pressure waveform over a continuous distending pressure. In most ventilators both the inspiratory and expiratory cycles are active i.e. gas is pushed in and pulled out. An alternative means of creating oscillation is by flow interruption.
During HFOV alveoli are kept open utilising a continuous distending pressure (the mean airway pressure: MAP) and not subjected to large pressure and volume swings causing the traumatic ‘inflate-deflate’ cycle to maintain gas exchange (Figure 1). In contrast during conventional ventilation the alveoli open and close on every breath delivered and large pressure swings (PIP/PEEP) are required to move relatively large volumes of gas to enable adequate gas exchange to occur.
Figure 1: Ventilation waveform in Conventional ventilation (PCV = Pressure Controlled Ventilation) and HFOV.
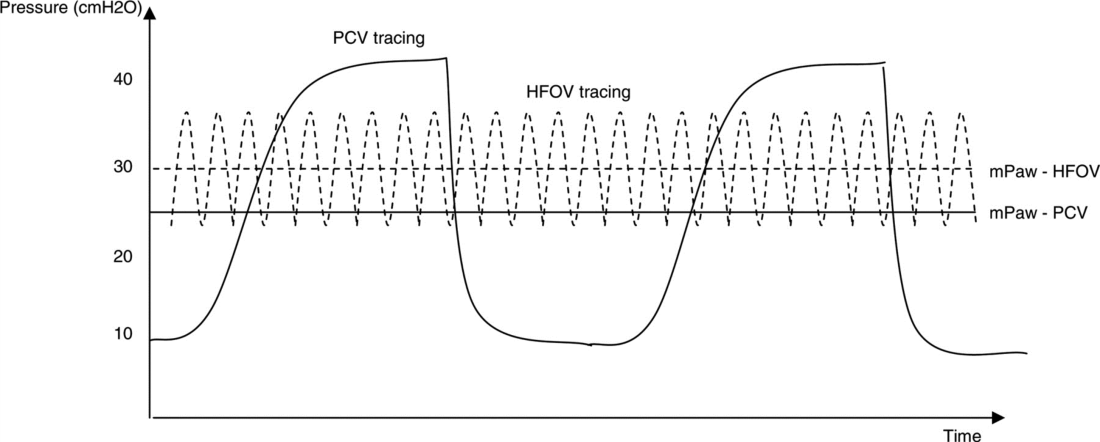
(Reproduced from Chan KP, Stewart TE, Mehta S. High-frequency oscillatory ventilation for adult patients with ARDS. Chest. 2007; 131(6):1907-1916.)
In HFOV oxygenation is decoupled from ventilation and each can be controlled independently. Oxygenation is determined by inspired FiO2 and lung recruitment, which is determined by MAP. Carbon dioxide clearance (i.e. ventilation) is controlled separately by the tidal volume which is dependent on oscillation frequency (oscillations per minute) and amplitude of the waveform ΔP (amplitude).
As per the Cochrane review (2015), there is evidence that the use of elective HFOV compared with CV results in a small reduction in the risk of CLD, but the evidence is weakened by the inconsistency of this effect across trials. Probably many factors, both related to the intervention itself as well as to the individual patient, interact in complex ways. In addition, the benefit could be counteracted by an increased risk of acute air leak. Adverse effects on short-term neurological outcomes have been observed in some studies but these effects are not significant overall. Most trials reporting long-term outcome have not identified any difference.
3.5 Mechanism of Gas Transport in HFOV
Gas transport in HFOV is thought to be complex and accomplished by a combination of the following mechanisms (see also Figure 2):
- Direct alveolar ventilation – ventilation by bulk flow to proximal lung units
- Pendelluft effect – The transfer of gas between lung units with different time constants i.e. transfer of gas from rapidly filling alveoli to slower filling alveoli
- Convective streaming – the shape of the stream of gas caused by rapid movement of gas forming an arrow shaped gas flow which penetrates the dead space
- Augmented (Taylor) dispersion - In the lungs, the branching network of the airways together with Pendelluft movement, leads to gas turbulence and mixing between the core and the periphery of the gas column and radial dispersion is eliminated. This results in greater gas mixing with lower tidal volumes.
- Cardiogenic mixing – the mixing of gas facilitated by the turbulence created in the airways by the pumping action of the cardiac muscle
- Molecular diffusion – the process by which molecules spread from areas of high concentration to areas of low concentration.
Figure 2: Proposed mechanisms of gas transport in HFOV
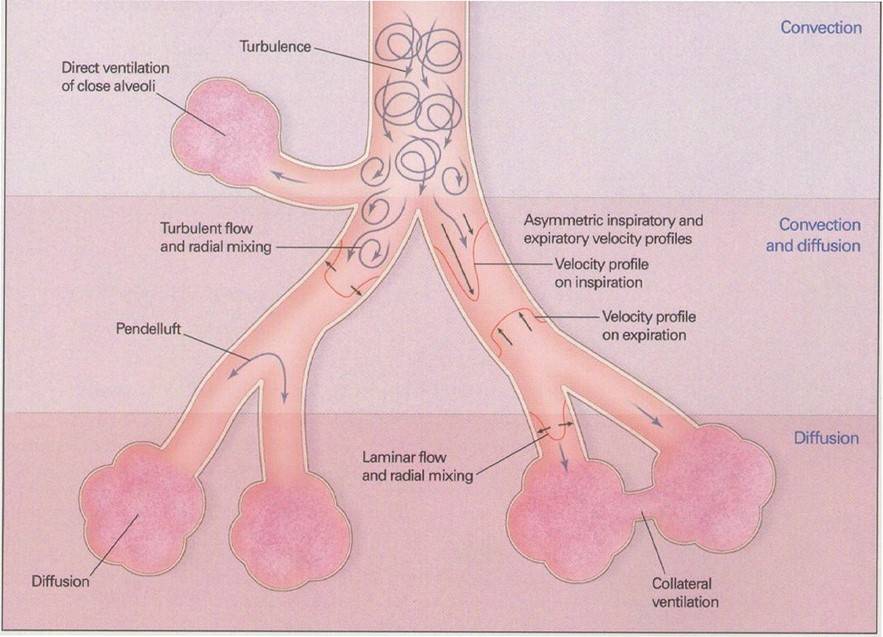
(Reproduced from Slutsky, AS, Drazen, JM Ventilation with small tidal volumes.N Engl J Med2002; 347,630-631)
It is important to appreciate that in HFOV the pressures set at the ventilator and delivered at the ET tube are not the same as those reaching the alveoli. Approximately 10% of the ΔP (amplitude) delivered at the endotracheal tube is transmitted to the terminal bronchioles and alveoli, compared with 90% of PIP transmission during conventional ventilation (Figure 3)
Figure 3: Reduction in HFOV waveform along respiratory tree
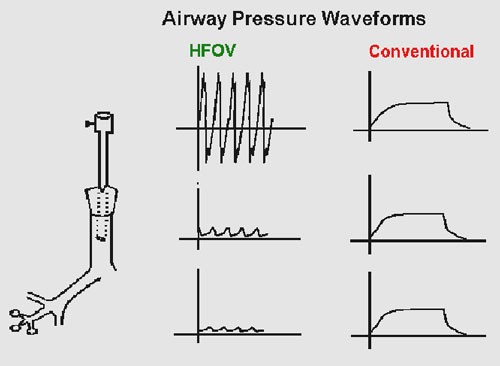
(Reproduced from Rajiv P K .Essentials of Neonatal Ventilation 2010)
3.6 Determinants of gas exchange in HFOV
The determinants of oxygenation and CO2 clearance (ventilation) during HFOV are discussed in detail below and summarised in Figure 4.
Figure 4: Ventilation parameters and effect on oxygenation and ventilation in HFOV and conventional ventilation (CMV)
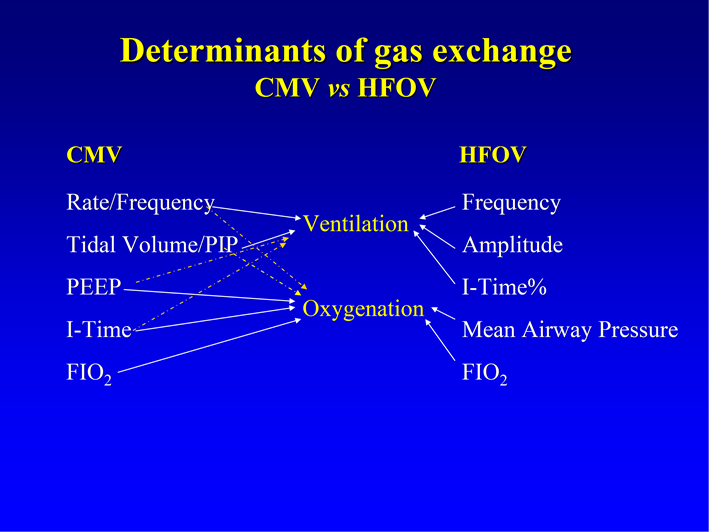
(Reproduced from Royal Children’s Hospital, Melbourne Newborn Services Guidelines – 2014)
Determinants of oxygenation in HFOV
Oxygenation is determined by lung volume and oxygen concentration delivered (FiO2). The mean airway pressure (MAP) setting on the HFOV is used to modify lung volume by recruiting atelectatic lung units and optimising the alveolar surface area for gas exchange. The MAP is considered to act as a continuous distending pressure (CDP) on the alveoli. The goal of recruitment manoeuvers in HFOV is to open atelectatic lung units to gas exchange and then find the lowest possible mean airway pressure to keep them open (see Optimal ventilation strategy below)
Determinants of ventilation (CO2 clearance) in HFOV
In conventional ventilation modes CO2 clearance is determined by minute ventilation which is: minute volume tidal volume x frequency. The HFOV equivalent of minute volume is the gas transport coefficient or DCO2.
During HFOV CO2 clearance is determined by the amplitude (ΔP) (amplitude) and frequency (measured in hertz):
- Amplitude (DP): The amplitude is created by the distance that the piston/diaphragm moves and is the peak to trough swing (oscillation) around the mean airway pressure. The movement created by this swing results in a gas volume displacement and a visual chest wiggle. The higher the ΔP (amplitude), the greater the displacement of gas i.e. tidal volume. An increase in DP (amplitude) should result in an increased tidal volume and increased removal of CO2.
- Frequency: Frequency is the number of cycles per minute: one hertz equals 60 cycles per minute. Decreasing hertz results in increased time for the oscillatory wave form cycle to be delivered thereby increasing tidal volume and improving CO2 Decreasing hertz will also result in less attenuation of the oscillatory waveform, generating more chest wall movement and increasing CO2 removal. This is in contrast to conventional ventilation where increases in rate cause increased tidal volumes and enhanced CO2 removal.
3.7 Optimal Ventilation Strategy
Successful application of HFOV is dependent upon ventilation with the lung recruited, known as the open lung strategy or the high lung volume strategy.
Continuous distending pressure (MAP) during HFOV recruits the lung if sufficient pressure is applied on initiation to open most lung units and retains volume if sufficient pressure is maintained to keep most lung units open. In other words, the goal of the open lung strategy is to open collapsed alveoli to gas exchange and then find the lowest possible MAP that will keep them open.
The ‘art’ of HFOV relates to achieving and maintaining optimal lung inflation. Optimal oxygenation is achieved by gradual increments in MAP to recruit lung volume and monitoring the effects on arterial oxygenation. The aim is to achieve maximum alveolar recruitment without causing over-distension of the lungs.
Optimising lung inflation with MAP: It is useful to conceptualise HFOV as like taking the lung around one sustained pressure volume hysteresis loop (Figure 5). Using the principles of P/V relationship, lung recruitment and and optimal range of lung volume we can apply these to optimise lung volume and oxygenation (Figure 6).
Figure 5: Pressure volume relationship in the lung demonstrating optimal pressure range with maximal lung recruitment (lung volume)
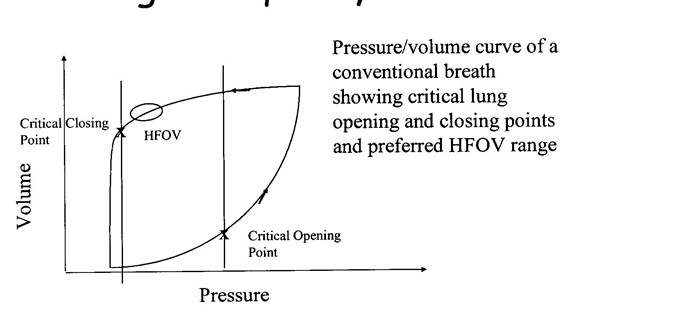
(Reproduced from Royal Children’s Hospital, Melbourne Newborn Services Guidelines – 2014)
Figure 6: Pressure volume relationship in the lung demonstrating different stages of lung inflations as detailed below as Point A,B,C and D
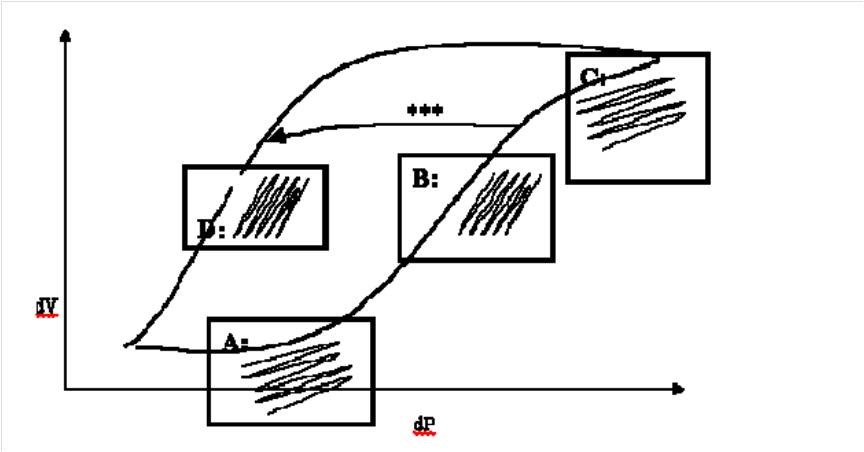
(Reproduced from Royal Prince Alfred Hospital, Sydney Newborn Services Guidelines – 2006)
Point A in figure: Under-inflation: At this point the lung is under-inflated, PVR will be high and relatively large amplitude will produce only small changes in volume. Clinically this manifests as a high oxygen requirement with limited chest vibration. CO2 clearance is also reduced.
Point B in figure: Optimal recruitment inflation: Once the lung has opened up with higher MAP, smaller amplitude will produce a larger change in volume. Clinically this manifests as improved oxygenation (falling oxygen requirements) and good chest vibration resulting in improved CO2 clearance. PVR will also be lower.
Point C in figure: Over-inflation: At this point excessive MAP has produced over-inflated lung. Oxygenation and CO2 clearance will start to deteriorate and PVR will increase contributing to cardiovascular compromise. This is the most dangerous point in HFOV and is to be avoided at all costs. It is difficult to pick clinically because the oxygen requirement may stay low, although they will eventually rise and the reduced chest vibration is easy to miss. Chest X-ray may be helpful to detect over-inflation.
Point D in figure: Optimal inflation: The goal should be to move the babies lungs from point B to point D avoiding point C (as shown on the arrow marked *** in Figure 2). Having achieved optimal lung inflation by slowly reducing MAP it should be possible to maintain the same lung inflation, oxygenation and ventilation at a lower MAP. If MAP is lowered too far oxygen requirements will start to rise again
Optimising ventilation:
- This is controlled mainly by adjusting amplitude (DP) to achieve optimal pCO2. Although the amplitude (DP) of each breath appears large by comparison to conventional ventilation pressures, the attenuation of oscillation through the endotracheal tube (ETT) means that the transmitted amplitude at the level of the alveolus is very small.
- Higher amplitude (ΔP) will increase tidal volume and hence CO2 removal.
- With increasing ventilator frequency, lung impedance and airway resistance increases so the tidal volume delivered to the alveoli decreases further. This contributes to the apparent paradox that increasing ventilator frequency may reduce CO2 elimination, leading to raised PaCO2 and vice-versa.
3.8 HFOV with Volume Guarantee (HFOV-VG):
HFOV-VG allows the clinician to set a predefined tidal volume, irrespective of other ventilator variables such as ‘frequency’ or ‘I:E ratio’. The clinician will define a maximum ΔP (amplitude), and the ventilator will adjust the delivered ΔP (amplitude) as required (up to the predefined ΔP/amplitude max) to achieve the set tidal volume.
HFOV-VG is still not widely used due to insufficient data in neonates. There are various studies on animal and experimental lung models but Belteki et al (2019) reported the first detailed analysis of ventilation parametres when using neonatal HFOV-VG over long periods. They stated that in contrast to the traditional HFOV, ventilator tightly controls the VThf while the ΔP (amplitude) varies widely when HFOV-VG mode is used. The use of targeted VThf with autochanging ΔP (amplitude) could be useful when the respiratory mechanics change rapidly such as after surfactant therapy, drainage of a pneumothorax or treatment with sedation and muscle relaxation. Without VG, these events could lead to excessive oscillations and hypocapnia, unless the ΔP (amplitude) is reduced promptly by the medical team. Despite good overall control in HFOV-VG, there is frequently short term variability of VThf, which could be secondary to patient- ventilator interactions i.e. baby’s spontaneous breathing activity or movements than on whether VG was used or not. Also, the strong inverse relationship between VThf & DCO2 with pCO2 in blood could not be established, therefore close monitoring of EtCO2 or pCO2 in blood during HFOV-VG was recommended.
They have suggested to start VThf at 2-2.5ml/kg with close monitoring of CO2 values. Once the patient is stable, it could then be weaned in small steps i.e. no more than 0.1ml/kg at a time. Gonzalez-Pacheo et al (2018) in their study on animals showed that use of very low VThf with high frequency (20 Hz) to maintain a target pCO2, significantly reduced the ventilator lung injury seen on tissue histology, when compared to the group using higher VThf and lower frequency(10hz).
This guideline has been developed with particular reference to the HFOV Guideline of the Newborn Intensive Care Unit, Royal Children’s Hospital Melbourne and clinical practice guideline for NICU KEMH, PCH and NETS Western Australia
Avila, K., Mazza, L., and Morgan-Trujillo.L. 1994. High Frequency Oscillatory Ventilation: A nursing approach to bedside care. Neonatal Network, 13 (5), 23-31.
Bouchut, J.C. Godard, J. & Claris, O. (2004) High Frequency Ventilation. Anaesthesiology, 100 (4), 1007-1012.
Bunnell, J.B. (1990) High-Frequency Ventilation in Newborn and Pediatric Intensive Care. Neonatal Intensive Care, May/June, 28-32.
Bunnell, J.B. (1990) High-Frequency Ventilation in newborn and Pediatric Intensive Care – Part ll. Neonatal Intensive Care, July/August, 12-18.
Chan KP, Stewart TE, Mehta S. (2007).High-frequency oscillatory ventilation for adult patients with ARDS. Chest; 131(6):1907-1916
Duval, E.L. Markhorst, D.G. & Vught, A.J. (2009) High frequency oscillatory ventilation in children: an overview. Respiratory Medicine CME 2, 155-161.
Froese, A.B. & Kinsella, J.P. (2005) High-frequency oscillatory ventilation: lessons from the neonatal/pediatric experience. Critical Care Medicine, 33(3), S115-S121.
Mammel MC. High-frequency ventilation. In: Goldsmith JP and Karotkin EH (Eds). Assisted ventilation of the neonate. 4th Edition, Saunders, pp 183-201
Pillow, J.J. (2005) High-frequency oscillatory ventilation: Mechanisms of gas exchange and lung mechanics. Critical Care Medicine, 33(3), S135-141.
Spitzer, A.R. (2005) Intensive Care of the Fetus and Neonate (2nd ed), Philadelphia, Elsevier Health Sciences.
Dimitriou G, Greenough A, Kavvadia V, Milner AD. (1999). Comparison of two inspiratory: expiratory ratios during high frequency oscillation. Eur J Pediatr. 1999 Oct;158(10):796-9.
Cools F, Offringa M, Askie LM. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants. Cochrane Database of Systematic Reviews 2015, Issue 3. Art. No.: CD000104.
Belteki G, Morley CJHigh-frequency oscillatory ventilation with volume guarantee: a single-centre experienceArchives of Disease in Childhood - Fetal and Neonatal Edition 2019;104:F384-F389.
González-Pacheco N, Sánchez-Luna M, Ramos-Navarro C, Navarro-Patiño N, de la Blanca AR. Using very high frequencies with very low lung volumes during high-frequency oscillatory ventilation to protect the immature lung. A pilot study. J Perinatol. 2016 Apr;36(4):306-10. doi: 10.1038/jp.2015.197. Epub 2016 Jan 7.
Last reviewed: 10 October 2020
Next review: 01 October 2023
Author(s): Tayyaba Yasmeen – Paediatric Trainee GG&C; Althaf Ansary - Neonatal Consultant – Ayrshire Maternity Unit
Co-Author(s): Other Professionals consulted: Neil Patel – Neonatal Consultant – QUEH
Approved By: West of Scotland Neonatology Managed Clinical Network