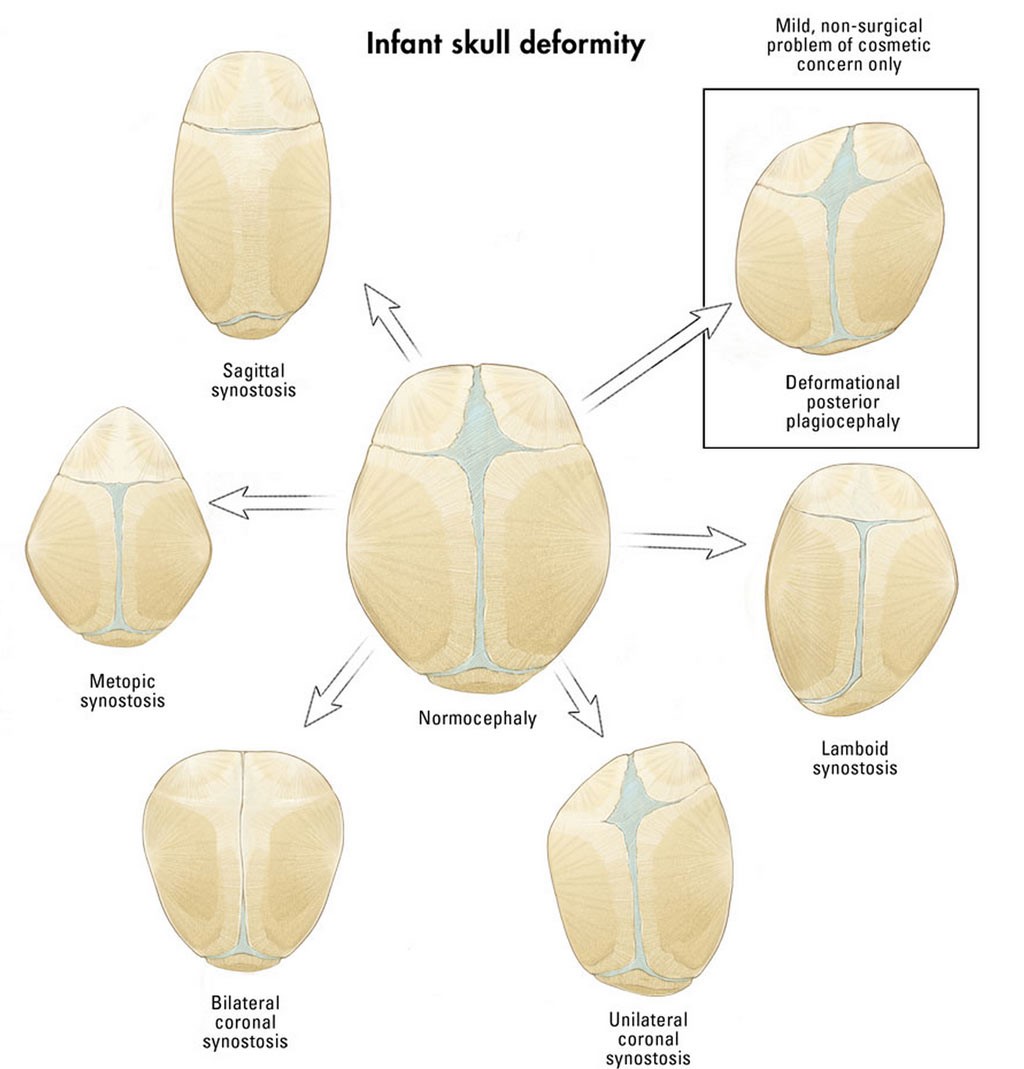
Sagittal craniosynostosis – Scaphocephaly
Sagittal craniosynostosis is the most common form of craniosynostosis involves the suture that runs from the front to the back of the skull, when fused early it creates a narrow elongated ‘boat shaped skull’. There may also be frontal bossing, occipital bullet/protuberance and ridging over the sagittal suture.
Metopic craniosynostosis – Trigonocephaly
The metopic suture is in the middle of the forehead running from top of head (from the baby’s soft spot or fontanelle) towards the nose, when this suture if fused it presents with narrow pointed forehead that has a triangular shape when viewed from above and there may be hypotelorism. The metopic suture naturally closes between 4-8 months of age and at this time there may be mild ridge (metopic ridge) evident however, this alone does not indicate metopic synostosis if the skull shape is not affected.
Unicoronal craniosynostosis – Anterior Plagiocephaly
Unicoronal craniosynostosis is where one of the coronal sutures at the front of the skull just in front of the ears have fused early, creating the appearance of an asymmetrical skull. The forehead appears flat on the affected side and protrudes (frontal bossing) at the non-affected side, the root of the child’s nose may deviate towards affected side, and there may be asymmetry of the eye position giving appearance of harlequin eye.
Bicoronal craniosynostosis – Brachycephaly
In bicoronal craniosynostosis, both of the coronal sutures are fused creating appearance of a short skull from front to back, there can be wide spacing between eyes and elongated forehead (upwards).
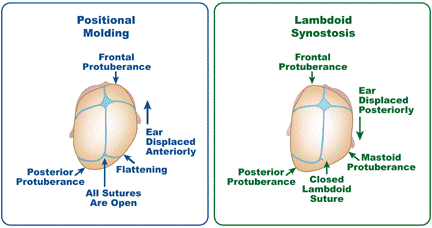
Lambdoid craniosynostosis – Posterior Plagiocephaly
Lambdoid craniosynostosis is the rarest type of craniosynostosis with flattened occipital (back) area & bossing (protruding) over the mastoid bone behind the ear on the affected side. The unaffected occipital area appears fuller and when the head viewed from above will show the affected side ear positioned backwards compared to the position of unaffected side ear.
Pansynostosis – Turreicephaly or Oxycephaly
This is where there is fusion of all or multiple sutures, causing restricted growth (small head circumference) and presents as a cone or turret shaped head.

 RHC for Health Professionals
RHC for Health Professionals