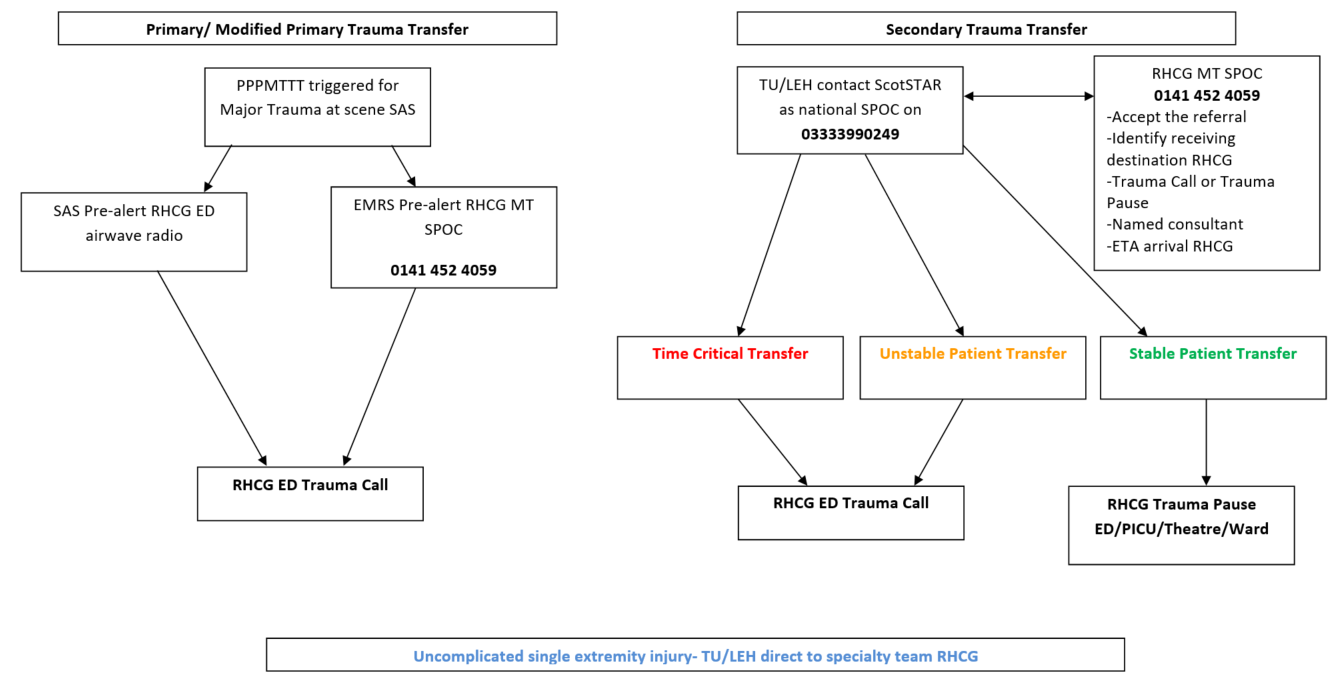
For any child that requires transfer from a TU/LEH for MTC level care at RHCG, the referring site will contact ScotSTAR as the national paediatric trauma SPOC as per guidance. The safety of the proposed transfer will remain the remit of the ScotSTAR clinician and not the RHCG SPOC.
The ScotSTAR clinician will bring in the RHCG SPOC, the consultant taking named responsibility (where possible) and any relevant specialty teams to a conference call for initial referral discussions. An automatic acceptance policy applies for these referrals as per the rest of the Scottish Trauma Network.
From these discussions the RHCG SPOC will:
- Accept the referral
- Establish the most appropriate destination for the child on arrival at RHCG
- Establish the most appropriate reception for the child, trauma call or pause
- Establish the clinician taking named responsibility for the patient at RHCG
- Establish the ETA at RHCG or request to be contacted with this once en route
The RHCG SPOC can leave the conference call once the above have been clarified. Clinical support and transfer advice can continue to be provided by the ScotSTAR clinician.
Secondary transfers (including patients that are intubated and ventilated) will fall into the following categories and be managed as follows:
a) Time Critical Transfers
- Will be transferred to RHCG by the referring site to ED at RHCG
- Will have a trauma team response in ED at RHCG
- The RHCG SPOC will assist with the organisation of any imaging and/ or blood products ahead of arrival in conjunction with the responsible team
b) Unstable Transfers
- Will be retrieved by ScotSTAR if non time critical to ED at RHCG
- Will have a trauma team response in ED at RHCG
- The RHCG SPOC will assist with the organisation of any imaging and/ or blood products ahead of arrival in conjunction with the responsible team
c) Stable Transfers (excluding single uncomplicated extremity injuries)*
- Will either be retrieved by ScotSTAR or arrive by paramedic transfer
- Can proceed directly to agreed destination e.g. PICU/ theatre, or be received in ED**
- Will require a trauma pause on arrival at the agreed destination at RHCG
*If the patient is more than 24 hours from admission and coming from an inpatient bed elsewhere for specialist input at RHCG they should be managed as per RHCG’s inter-hospital transfer policy.
** If the patient is to go directly to a destination other than ED in RHCG, the named responsible consultant must be in agreement with this.
d) Stable, uncomplicated single extremity injuries (including fractured femurs)
- Do not require discussion with ScotSTAR as national SPOC or with RHCG SPOC
- Should be a direct specialty to specialty referral
- Should be reviewed on arrival in ED or inpatient bed by the accepting specialty as per the inter-hospital transfer policy**
- A trauma pause can be arranged by the accepting specialty on arrival at the agreed destination at RHCG if deemed appropriate.


 GGC Paediatric Guidelines
GGC Paediatric Guidelines