Chest drain insertion is a procedure that is performed by the doctor or ANP in paediatric critical care. However, it is important that the nurse, as well as the physician/ANP inserting the drain, has an understanding of not only the benefits but the risks of such a procedure. It is recommended that all personnel involved with insertion of chest drains be suitably trained and supervised. As such it is recommended that all nursing staff have an understanding of the concepts of chest drainage including the following: anatomy, respiration, indications for chest drainage, risks and ongoing care and management.
Risks: The decision to insert a chest drain is based on clinical findings and patient need and, may be urgent. However, where possible it is prudent to adequately prepare the patient for the procedure. This includes discussion with child and parents, consideration of what sedation, analgesia and anaesthesia may be required, patient positioning and correction of blood clotting or platelet counts.
Sutures: Much of the literature supports the use of a non-absorbable suture (silk) to secure the drain in place and another to close the incision wound once the drain is removed. Physicians/ANP’s should use a suture as recommended as per the PICU Medical Chest Drain Insertion protocol (separate document pending).
Practical chest drainage system issues: When there is no air leak, the water level in the water seal chamber should rise and fall with the patient's respirations, reflecting normal pressure changes in the pleural cavity during respiration. During spontaneous respirations, the water level should rise during inhalation and fall during exhalation. If the patient is receiving positive pressure ventilation, the oscillation will be just the opposite. Oscillations may be absent if the lung is fully expanded and suction has drawn the lung up against the holes in the chest tubes.
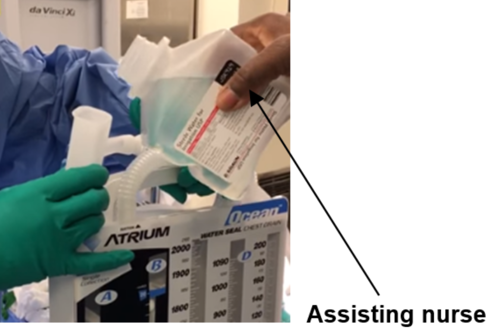
A patient with mediastinal chest tubes (and a ‘closed’ chest) should have no bubbling or fluctuations in the water seal chamber. As one of the risks of accumulation of fluid, blood or clots around the heart is cardiac tamponade, it is particularly important for nurses caring for patients with mediastinal chest tubes to be watchful for signs of cardiac tamponade with special attention paid to the volume and consistency of drainage in the collection chamber (D) (Fig. 3).


 GGC Paediatric Guidelines
GGC Paediatric Guidelines