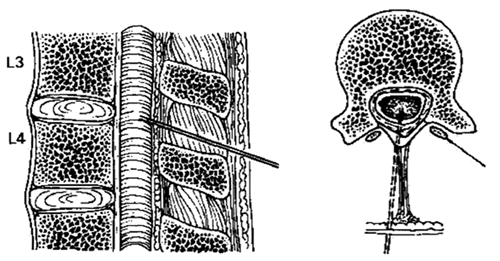
This document is intended to inform the practice of oncologists, anaesthetists & anaesthetic assistants performing percutaneous neuraxial procedures
There has been some discussion in the medical literature about recent cases of adhesive arachnoiditis and the role of different skin prep solutions. Contamination of equipment with small droplets of cleaning solution has been implicated. The numbers of cases are small and it’s difficult to draw firm conclusions, however from the evidence available we can agree on some learning points from these case reports;
Do Notpour chlorhexidine in alcohol solution onto an epidural / spinal tray. This risks contamination of equipment with droplets from a splash.
Do Notspray chlorhexidine in alcohol anywhere near an uncovered epidural / spinal trolley. Keep trolleys covered / well away from site being prepped.
Do Not put any swabs used for cleaning back on the trolley
Doalways let the skin prep dry fully before touching the skin.
Do check gloves after prepping & if skin prep is on gloves, change before handling epidural / spinal equipment
To adequately prep the skin you may:
Spray the skin with 0.5% chlorhexidine in alcohol (or ask assistant to do this for you)
Use a ‘chloraprep’ 2% chlorhexidine with alcohol swabstick
Chlorhexidine is a more effective skin preparation than Iodine solutions for these procedures
Further Information:
Bogod D. The sting in the tail: antisepsis and the neuraxis revisited. Editorial in Anaesthesia67: 12, December 2012
Prepared by Dr Graham Bell on behalf of the Anaesthetic Advisory Group 5th December 2012.


 GGC Paediatric Guidelines
GGC Paediatric Guidelines