

 GGC Paediatric Guidelines
GGC Paediatric Guidelines
|
PN |
Parenteral Nutrition |
|
IV |
Intravenous |
|
GOR |
Glucose Oxidation Rate |
|
RQ |
Respiratory Quotient |
|
EFA |
Essential Fatty Acid |
|
SMOF |
Soya, Medium chain, Olive oil, Fish oil intravenous lipid blend |
|
BSPGHAN |
British Society of Paediatric Gastroenterology, Hepatology & Nutrition |
|
ESPGHAN |
European Society of Paediatric Gastroenterology, Hepatology & Nutrition |
|
NEC |
Necrotising Enterocolitis |
|
NICE |
National Institute for Health and Care Excellence |
|
UVC |
Umbilical Venous Catheter |
|
AREDF |
Absent/ Reduced End Diastolic Flow |
|
VLBW |
Very Low Birth Weight Infant |
|
ELBW |
Extremely Low Birth Weight Infant |
|
NCEPOD |
National Confidential Enquiry into Patient Outcome and Death |
|
PNALD |
Parenteral Nutrition Associated Liver Disease |
|
IUGR |
Intra-Uterine Growth Retardation |
|
IVC |
Inferior Vena Cava |
|
SVC |
Superior Vena Cava |
|
PAU |
Pharmacy Aseptic Unit |
Parenteral feeding of preterm and term infant

Objectives
This guideline is applicable to all medical, nursing, dietetic and pharmacy staff caring for babies requiring parenteral nutrition (PN). It covers parenteral nutrition (intravenous feeding) for babies born preterm, up to 28 days after their due birth date and babies born at term, up to 28 days after their birth. It aims to:
- Ensure the safe provision of parenteral nutrition
- Promote and maintain optimal growth and development
- Help reduce the risk of deficiencies in nutritional intake
Audience
This guideline is applicable to all medical, nursing and pharmacy staff caring for infants in neonatal units in the West of Scotland.
This guideline is applicable to all medical, nursing, dietetic and pharmacy staff caring for babies requiring parenteral nutrition (PN). It covers parenteral nutrition (intravenous feeding) for babies born preterm, up to 28 days after their due birth date and babies born at term, up to 28 days after their birth. It aims to;
- Ensure the safe provision of parenteral nutrition
- Promote and maintain optimal growth and development
- Help reduce the risk of deficiencies in nutritional intake
Appropriate nutrition is essential for growth and development (1-3). Neonates who are unable to tolerate adequate enteral nutrition will require PN. Total parenteral nutrition (TPN) describes a situation whereby all nutrition is delivered intravenously however PN is often used in the neonatal unit in conjunction with enteral feeds either to maintain nutritional intake as milk feeds are increased, or for babies in whom full enteral intake is not tolerated (e.g. short gut). For the purpose of this guideline, the term PN will cover both partial and total parenteral nutrition.
PN administration should be based on nationally agreed evidence based guidelines, recognising that the evidence base for neonatal PN can be limited (4,5). To date there has been no randomised controlled clinical trial of neonatal PN powered to examine longer term outcomes including neurodevelopment and cardiovascular health. The recently published National Institute for Health and Care Excellence (NICE) guideline for neonatal parenteral nutrition (6) forms the basis of this guideline which should be used in conjunction with clinical judgement.
PN should be considered in any neonate who is unlikely to meet their nutritional requirements via the enteral route, either due to immaturity or illness. Premature infants, and especially those of extremely low birth weight are particularly vulnerable due to their low nutritional reserves (8). Early provision of nutrition for preterm infants is associated with improved weight gain and head growth (9). When a baby meets the indications for parenteral nutrition, start it as soon as possible, and within 8 hours at the latest.(6) This should ideally follow confirmation of umbilical venous catheter (UVC) or long-line placement (10) but PN should not be delayed if there is only peripheral access. Table 1 provides specific indications for PN prescribing.
Table 1: Indications for parenteral nutrition in neonates
|
Absolute Indications |
< 31 completed weeks’ gestation and/or < 1.25 kg birth weight Congenital gastrointestinal defects (e.g. gastroschisis, intestinal atresia, congenital diaphragmatic hernia) Inability to tolerate enteral nutrition for a period likely to result in a significant nutritional deficit |
|
Relative Indications |
Infants ≥31 weeks gestation or ≥ 1.25kg who are not expected to receive adequate enteral feeds(e.g. severe intra uterine growth restriction with associated absent or reduced end-diastolic flow |
|
Indications for starting neonatal parenteral nutrition if enteral feeds are stopped |
For Preterm babies
For term babies
|
During the first 24 – 48 hours of life, fluid shifts from the extra-vascular to intra-vascular compartment and initial oliguria is followed by a diuretic phase with associated weight loss of up to 10%. The subsequent increase in both water and electrolyte requirements may be very marked in the preterm infant, and requires that close attention is paid to fluid and electrolyte balance, particularly for the smallest babies. Small preterm babies typically require mostly water replacement in the first 24 to 48 hours, but thereafter sodium excretion in the urine increases and sodium supplementation is required. (10,11).
Measured fluid balance is notoriously inaccurate and accurate assessment of insensible losses is impossible. Importantly, measuring a negative fluid balance during the period of physiological diuresis should not necessarily prompt additional fluid replacement. The best method of assessing overall fluid balance is by weighing the baby; daily weight should be used in conjunction with regular biochemistry (8 – 12 hourly for the most unstable babies) and clinical assessment to determine daily fluid and electrolyte provision. It must be remembered that, although related, fluid balance and nutrition are not synonymous. The use of humidified double wall incubators reduces insensible water losses and subsequent fluid needs in preterm infants whereas the use of radiant warmers or single wall incubators may increase water loss and impair thermoregulation.
Suggested fluid and electrolyte requirements are documented in Tables 2 and 3. These are intended as guidelines only.
Table 2: Suggested total Fluid requirements ( Parenteral nutrition and other fluids)
|
Day of life |
Babies at risk of: |
Other babies |
|
Day 1 |
90 ml/kg/day |
75 ml/kg/day |
|
Day 2 |
105 ml/kg/day |
90 ml/kg/day |
|
Day 3 |
120 ml/kg/day |
105 ml/kg/day |
|
Day 4 |
135 ml/kg/day |
120 ml/kg/day |
|
Day 5 |
150 ml/kg day |
135 ml/kg/day |
|
Day 6 |
165 ml/kg/day |
150 ml/kg day |
|
Day 7 |
165-180 ml/kg/day |
150-165 ml/kg/day |
Reasons to exceed predicted fluid requirements
- Increased fluid losses, including polyuria
- Dehydration
- Extremely low birth weight babies (<1000g)
- (sometimes) hypoglycaemia with very high glucose requirement
Reasons for lower than predicted fluid requirements
- Acute renal injury - indicated by oliguria/anuria +/- rising creatinine
- Inappropriate ADH secretion - typically following asphyxia (increased weight with low plasma sodium concentration)
Table 3: A guide to electrolyte requirements
|
Parenteral electrolyte requirements |
Early (≤ 48 hours) |
Late |
|
Sodium |
||
|
<1.5kg infant |
0-3 mmol/kg |
3-5 mmol/kg * |
|
≥1.5kg infant |
0-3 mmol/kg |
3-5 mmol/kg |
|
Term (>35 weeks) |
2-3 mmol/kg |
2-3 mmol/kg |
|
Potassium |
||
|
<1.5kg infant |
0-2 mmol/kg |
2-5 mmol/kg |
|
≥1.5kg infant |
0-2 mmol/kg |
2-5 mmol/kg |
|
Term (>35 weeks) |
1.5-3mmol/kg |
1.5-3mmol/kg |
|
Chloride |
||
|
<1.5kg infant |
0-5 mmol/kg |
2-5 mmol/kg |
|
≥1.5kg infant |
0-5 mmol/kg |
2-5 mmol/kg |
- Many ELBW babies will require more sodium than this to account for renal losses
Recommendations
- Close monitoring of plasma sodium concentration and regular weighing are required in order to anticipate changing fluid and electrolyte requirements, particularly in extremely low birth weight babies.
The goal is to initiate nutritional support as soon as possible and achieve early energy accretion. Energy intake impacts directly on nitrogen balance and although the minimal energy needs of infants may be met with 50 - 60 kcal/kg/day, 100 – 120 kcal/kg/day (including 85 – 105 non-protein kcal/kg/day) is required to facilitate protein accretion (13-15).
Recommendations (6)
- If starting parenteral nutrition in the first 4 days after birth:
- give a starting range of 40 to 60 kcal/kg/day
- gradually increase (for example, over 4 days) to a maintenance range of 75 to 120 kcal/kg/day.
- If starting parenteral nutrition more than 4 days after birth:
- give a range of 75 to 120 kcal/kg/day.
Early amino acid (protein) introduction is essential if the high accretion rates seen in utero are to be matched and large deficits in the first week of life avoided (2). Evidence suggests it is safe to commence amino acid immediately after birth without metabolic complications (13, 16-18).
Estimates of amino acid requirements in preterm infants are based on the quantity required to achieve a positive nitrogen balance (1 g of nitrogen = 6.25 g of protein). The preterm infant excretes between 0.6 - 1.1 g/kg of protein per day. A minimum amino acid intake of 1.5 g/kg/day is required to prevent significant deficit (29, 30). The energy: nitrogen ratio is important and should be between 20 and 30 kcal non-nitrogen energy per g amino acid (6). The published literature supports amino acid intakes of 4 g/kg/day for preterm and 3 g/kg/day for term infants. Preterm infants should be commenced on 1.5 - 2 g amino acid/kg/day as soon as possible after birth (6). It should be borne in mind that target parenteral protein intake has been rarely achieved in the past.
In addition to the nine essential amino acids in adults (leucine, isoleucine, valine, lysine, methionine, phenylalanine, threonine, tryptophan and histidine), it is likely that taurine, tyrosine and cysteine are essential during infancy. Alanine and proline may also be ‘semi-essential’. The neonate also has a limited ability to metabolise an excessive intake of phenylalanine and tyrosine, which may have adverse implications for appropriate neurotransmitter formation).
Vaminolact is the nitrogen solution currently used for neonates in the West of Scotland. The amino acid profile (based on breast milk protein) includes cysteine, taurine and tyrosine, essential for premature neonates.
Note: most papers, and the NICE guidance, refer to requirements in terms of amino acid, rather than protein. 1g amino acid is equivalent to 0.89g protein
Recommendations (6)
- Parenteral amino acid provision should commence as soon as possible after birth.
- Parenteral amino acid provision should commence at a minimum of 1.5 - 2g/kg/day, increasing to a maximum 4 g/kg/day for preterm and 3 g/kg/day for term infants. If starting parenteral nutrition more than four days after birth give a range of 3 – 4g amino/kg (preterm) or 2.5-3g amino acid/kg (term)
- Energy: amino acid ratio must not be less than 20 kcal/g amino acid. Consider lower protein doses in patients with severe renal impairment
Carbohydrate in PN is prescribed as glucose (1g glucose = 10ml glucose 10% - 3.4 kcal). Glucose serves as the primary source of energy for the brain, renal medulla and erythrocytes and as metabolic fuel for muscle, liver, heart, kidney and the gut. (5).
Regardless of gestation, the initial quantity of glucose should be between 6 -9g/kg/day (4.2 – 6.3 mg/kg/min). This equates to 60 - 90 ml/kg/day of 10% glucose solution. Glucose provision should be increased gradually as tolerated (by approximately 2 – 3 g/kg/day) with attention paid to glucose provided by other sources, e.g. other IV infusions. The maximum glucose provision should be 16g/kg/day (11.1mg/kg/min)), but this may not be tolerated by the smallest preterm babies.
Care must be given not to provide glucose over and above the GOR as this leads to excess CO2 production and an increase in the Respiratory Quotient (RQ). This in turn promotes lipogenesis and fat deposition, particularly in the liver.
Hyperglycaemia is a recognised complication of preterm PN which can be managed either by reducing the amount of glucose provided, or by use of an insulin infusion. The use of insulin should be limited to situations where reasonable adaptation of glucose infusion rate, including continuous infusions, does not control hyperglycaemia (6). Refer to the West of Scotland Hyperglyaemia in the Neonate guideline for treatment of hyperglycaemia
Recommendations (6)
- Glucose infusion should commence at a minimum of 6-9g/kg/day (4.1 – 6.3 mg/kg/min, regardless of gestation
- Maximum glucose intake should not exceed1 mg/kg/min (16 g/kg/day) in the neonatal period.
Lipid administration is important because:
- It is a concentrated source of calories
- It prevents the development of essential fatty acid (EFA) deficiency.
- It is a vehicle for fat soluble vitamins
Lipid has historically been provided as a soy-bean oil-based emulsion (e.g. Intralipid20%). Intralipid provides essential and non-essential long-chain fatty acids for energy metabolism. However a newer lipid emulsion SMOFLipid is now the preferred product (see below).
SMOFLipid (Soya bean [30%], Medium chain triglyceride [30%], Olive oil [25%], and Fish oil [15%]) is a complex mixed-type emulsion. It has the advantage of containing fish oil but also provides EFA, in contrast to pure fish-oil based lipids. A number of studies have shown that SMOFLipid is as safe as the traditionally used soy-bean oil-based lipid emulsion (29-31) and a growing evidence base suggests that it has a role in the prevention and / or reversal of PN associated liver disease (PNALD) (27-29). This is reflected in the NICE recommendation that fish oil containing lipid should be considered in infants with parenteral nutrition associated liver disease.
EFA deficiency can develop within two to three days in the preterm infant who does not receive an adequate infusion of lipid (19). Preterm minimum EFA requirements are 0.25 g/kg/day linoleic acid (met by 0.5 g [2.5ml]/kg/day Intralipid 20% or 1.5 g [7.5ml]/kg/day SMOFLipid). The normal maximum lipid requirement is 3.5g/kg/day for preterm infants and term infants. Up to 4g/kg can be given for individual patients following discussion (6) Intravenous lipid is isotonic with blood and may be infused peripherally; it helps to maintain vein patency.
The evidence base for the gradual introduction of lipid is limited but step wise increases allow for the monitoring of hypertriglyceridaemia, and ensures an appropriate ratio of fat calories to total calories (25-40% of non-protein calories). Previous concerns that the early introduction of lipid infusions worsens chronic lung disease, sepsis, hyperbilirbinaemia, etc., have not been confirmed (19,20).
Serum triglyceride (TG) levels should be monitored following any increase in lipid dose and in those receiving lipid doses > 3 g/kg/day. Critical illness, including sepsis, may impair lipid metabolism and TG levels should be monitored daily with a low threshold for reducing the lipid dose (see table 6) (6).
- An unlicensed preparation – SMOFvits – is available which incorporate both water and fat soluble vitamins and ensures that patients receive vitamins when commenced on PN out of hours. Note that the maximum licensed dose is 3 g/kg/day. This is the preferred first line option for lipid administration
Recommendations (6)
- Intravenous lipids should commence as soon as possible on the first day of life at a dose of 2 g/kg/day.
- Lipid must be commenced at the same time as aqueous PN to ensure appropriate nutrition.
- Lipid should be incremented by 0.5-1 g/kg/day with reference to triglyceride levels (see monitoring section).
- Preterm infants should receive a minimum 0.25 g/kg/day linoleic acid in order to prevent EFA deficiency (met by 1.5 g/kg/day SMOFLipid).
- Normal nmximum lipid provision should be 3.5 g/kg/day in preterm and term infants.
- Use SMOFLipid as first line lipid administered over 24 hours. Consider cycling lipid over 20 hours in the following infants;
- Infants at high risk of needing PN for >28 days
- PN dependent >28 days even if liver function tests are normal.
- Significant liver dysfunction before 28 days on PN; evolving conjugated hyperbilirubinaemia or clinical signs of cholestasis (pale stools, dark urine)
8.1 Vitamins
The optimal parenteral vitamin requirements for preterm infants have never been determined. Current recommendations are therefore based on small, historical studies and expert opinion (Table 4) (6,7). The provision of fat and water soluble vitamins is limited by the availability of commercial preparations.
An adequate supply of vitamins is essential for growth and development. Preterm infants may have low or borderline body stores of fat soluble vitamins secondary to limited placental transfer and these should be supplied as soon as possible. Water soluble vitamins must be administered regularly as they are not stored in any significant amounts. Vitamins should be supplied in the lipid phase of PN.
Vitamins administered intravenously can adhere to delivery tubing and may be degraded by light (see administration section). As a result the actual amount delivered to the infant may be significantly lower than the intended dose.
The regimens stated on the PN prescription sheets automatically add the appropriate amounts of Peditrace, SolivitoN and Vitlipid N Infant (Table 5).
8.2 Minerals and trace elements
The individual requirements for minerals and trace elements also remain a matter of debate (Table 4) (6). Trace elements are involved in enzymatic activities and immunological reactions and preterm infants are at risk of trace element deficiency secondary to low body stores at birth and the high demands of rapid growth. Parenteral mineral and trace element recommendations are calculated to prevent the development of deficiency syndromes and to match in-utero accretion rates (22).
Iron is not routinely provided in neonatal PN and is not a component of commercially available trace element preparations. Concerns exist regarding iron overload and the role intravenous iron can play in the impairment of immune function and the increase in infection risk secondary to bacterial overgrowth.
Table 4: Vitamin, mineral and trace element requirements for preterm infants (ESPGHAN)
|
Fat soluble vitamins (dose/kg/day) Vit A (microgram RE)150 – 300 ** Vit D (microgram) 0.8 Water soluble vitamins (dose/kg/day) Ascorbic Acid (mg) 15-25 |
Minerals & trace elements (dose/kg/day) Molybdenum (microgram) 1 |
Table 5: Recommended vitamin and mineral additives (Kabi Fresenius product data)
|
Nutrients |
Product |
Dose |
|
Fat soluble vitamins |
Vitlipid N Infant |
4ml/kg/day up to 2.5kg |
|
Water soluble vitamins |
Solivito N |
1ml/kg/day |
|
Trace elements |
Peditrace |
1ml/kg/day |
Recommendations
- Preterm infants receiving PN should receive parenteral vitamins, minerals and trace elements ideally from the outset, but as soon as possible after starting PN, as per tables 4 and 5.
- If using SMOFvits water and fat soluble vitamins will be present in the lipid and further additions are not necessary
In preterm infants the retention of calcium (Ca) and phosphorus (PO4) is proportional to growth (23). Fetal bone mineral accretion rates of 2 mmol Ca and 1.52 mmol PO4 per 100g newly grown body weight can be achieved if the infant receives adequate quantities of both minerals (24). These figures are therefore used as the reference mark for Ca and PO4 PN requirements for preterm infants (6).
ELBW babies will require ≥2mmol PO4/kg/day.
Recommendations
For preterm and term babies, give phosphate as follows:
- If starting parenteral nutrition in the first 48 hours after birth:
- give 1 mmol/kg/day
- increase to a maintenance dosage of 2 mmol/kg/day after 48 hours.
- If starting parenteral nutrition more than 48 hours after birth, give 2 mmol/kg/day.
- Give a higher dosage of phosphate if indicated by serum phosphate monitoring.
Individualised (or bespoke) PN provision has generally been considered the “gold standard” for achieving optimal nutrient intake. However few studies have actually assessed the most effective way to provide PN in the clinical setting. The 2010 National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report identified good neonatal PN practice in only a quarter of patients, with a third of neonates receiving inadequate PN for their nutritional needs (3, 25, 26). As a consequence of these findings there has been a move towards standardisation of neonatal PN. The aim is that with careful attention to local workload, PN formulations and prescribing practices, the majority of infants can be managed using standardised regimens.
Through removing the need for multiple additions during the compounding process standardisation may lower the risk of error by encouraging the advance preparation of solutions by pharmacies and commercial providers, facilitating end product testing and quality assurance interventions (4).
Most difficulties associated with the use of standardised PN solutions relate to variations in electrolyte (especially sodium) requirements rather than macronutrient requirements. Providing access to standardised PN formulations that allow for some flexibility in electrolyte prescription can help to overcome these difficulties.
Recommendation:
- Standard PN solutions should be used wherever possible in order maximise nutrient delivery and to minimise the risk of errors in prescription and compounding.
1.0 Prescribing and Compounding
2.0 Monitoring of Parenteral Nutrition
2.2 Electrolyte monitoring and adjustment
2.3 Triglyceride Monitoring
3.0 Administration
4.0 Weaning of PN
1.0 Prescribing and Compounding
1.1 The decision to initiate PN should be made by a senior clinician (4) following the guidance in Table 1.
1.2 The standardised Scottish Neonatal bag should be used as the first line option as per local policy A sodium free bag is available for babies <28 weeks gestation for initial use. Electrolytes may be tailored to specific requirements by local Pharmacy Aseptic Units (PAU). Individualised PN should only be used where there is no suitable standardised formulation due to unusual nutrient and / or electrolyte requirements or severe fluid restriction. Care should be taken to ensure the prescription meets published recommended nutrient intakes wherever possible (3, 4, 5).
1.3 Prescription of PN should be performed by the clinical team caring for the patient. Ideally this should involve as a minimum a senior clinician and neonatal pharmacist (4).
1.4 PN can be ordered to cover a 48 hourly period in stable neonates but may be ordered daily in unstable neonates with frequently changing electrolyte requirements. The volumes to be administered require to be prescribed daily on the fluid charts.
1.5 The volume of PN prescribed will depend on overall fluid requirements, other infusions (IV medications) and enteral feed volumes. Priority should be given to maximising PN volumes in order to maximise nutritional intake.
The standard PN solution with appropriate lipid is likely to achieve target intake and can be infused peripherally in the absence of a central line. Additional continuous infusion will impact on total nutritional intake
Central line access
PN solutions with a glucose content greater than 12.5% must be infused via a central line
Peripheral access – standard formulation or sodium free
PN can make up full fluid volume if necessary
1.6 The correct body weight should be used for PN dosing. The weight of the baby often falls over the first two weeks of life and for this period the birth weight should be used as the working weight. Once birth weight is reached again, it is important to amend the prescription if the working weight is increased. If the baby is very oedematous the working weight may be less than the actual weight. The working weight should be reviewed each day on the ward round.
1.7 Any change in infusion rate must be clearly documented and the impact of this change on electrolyte intake considered.
2.0 Monitoring of Parenteral Nutrition
Serious and unexpected biochemical instability as a consequence of PN is rare, but can be potentially fatal. Routine biochemical monitoring against an agreed protocol which takes account of length of time on PN, prematurity, co-morbidities and other administered medicines is therefore essential (4).
Below is a suggested schedule of monitoring based on NICE and ESPGHAN recommendations for practice (6,7). Requirements may differ for individual infants and situations.
| First week of PN |
Stable PN |
||||||
|
|
Daily |
Twice |
Weekly |
Daily |
Twice weekly |
Weekly |
Monthly long term PN |
|
Review Infusion site |
hourly |
|
|
hourly |
|
|
|
|
Fluid balance ± weight |
√ |
|
|
√ |
|
|
|
|
Blood glucose |
6-8 hourly* |
|
|
√* |
|
|
|
|
U&E |
√ ** |
|
|
|
√ |
|
|
|
Calcium, Phosphate |
√ |
|
|
|
√ |
|
|
|
Magnesium |
√ |
|
|
|
√ |
|
|
|
Triglyceride (see below) |
√ |
|
|
|
|
√ |
|
|
LFTs |
√ |
|
|
|
√ |
|
|
|
Albumin |
√ |
|
|
|
√ |
|
|
|
Bilirubin |
√ |
|
|
|
√ |
|
|
|
Acid base balance |
√ |
|
|
√ |
|
|
|
|
Full blood count |
√ |
|
|
|
√ |
|
|
|
Trace elements (Zn Cu Mn Se) |
|
|
|
|
|
|
√ *** |
|
Vitamin A, D, E |
|
|
|
|
|
|
√ *** |
|
Growth (OFC) |
|
|
√ |
|
|
√ |
|
* Measure blood glucose level
- 1 to 2 hours after first stating parenteral nutrition and
- 1 to 2 hours after each change of parenteral nutrition bag
** ELBW, or babies with significant renal impairment, may require U&E levels two to three times daily.
*** Trace element and vitamin levels are difficult to interpret if acute phase reactants are elevated.
Measure electrolyte blood concentrations more frequently if the baby has previously had levels outwith normal ranges, doses have changed or there are clinical reasons for concern
2.2 Electrolyte monitoring and adjustment
- Chloride should be kept to a maximum of 3 mmol/kg/day to avoid causing or exacerbating acidosis, which can also lead to calcium and phosphate losses. Additional acetate to that already in the standard bag can be requested for patients with a high or rising chloride in order to reduce the chloride content of the PN.
- Check the sodium content of other infusions running especially as some infusions may be running in 0.45% saline and this can often be significant (0.9% sodium chloride contains approximately 150 mmol/litre of sodium).
- Be aware that a high potassium level may be the result of a haemolysed sample and not a true indication of plasma potassium. If renal output is good, the most likely reason for high plasma potassium is a haemolysed sample.
- Aim for high phosphate levels: 1.8 – 2.6mmol/L.
Electrolyte adjustment
Potassium – only in severe acute hypokalaemia and after discussion with consultant
Refer to the West of Scotland Potassium Chloride monograph for details on the administration of supplemental potassium
Sodium
Refer to the West of Scotland Sodium Chloride monograph for details on the administration of supplemental sodium
Calcium / Magnesium
Prepare a separate infusion as per neonatal IV drug monograph
2.3 Triglyceride Monitoring
Triglyceride (TG) levels should be monitored with each increase of 1 g/kg/day in lipid dose and weekly after the maximum dose is achieved and tolerated (6). More frequent monitoring may be required if the infant is receiving high lipid doses (>3 g/kg/day), or becomes critically unwell e.g. with sepsis. Septic children have a decreased rate of fat elimination which in turn may cause increased insulin resistance and hyperglycaemia (6). Interventions based on triglyceride levels are documented in Table 6.
Table 6: Suggested lipid intake based on triglyceride level
|
Trig Level |
IV Lipid Intake Prescribed (for infusion) |
|
<3.0mmol/L |
- Advance lipid intake as normal. |
|
≥3 mmol/L |
Stop lipid infusion for 24 hours and remeasure TG level. |
The figure of 3mmol/L is not an absolute figure. Consider trends and clinical circumstances when adjusting doses
Recommendations:
- All infants on PN should receive consistent regular monitoring.
- Triglycerides should be monitored with each increase of 1 g/kg/day of IV lipids and twice weekly after the maximum dose is achieved and tolerated.
- More frequent monitoring may be required if the infant is receiving high lipid doses (>3g/kg/day), or if the infant becomes critically unwell e.g. with sepsis
- Consideration should be given to monthly monitoring of trace elements and fat soluble vitamin levels in infants likely to require long term PN (>28 days) with minimal or no enteral feeds.
3.0 Administration
3.1 Prolonged PN administration should be via a central line (6, 16); either a UVC, a surgically inserted central line (CVL) or a peripherally inserted central catheter (PICC). Where UVC are used they should generally not be left in place for more than 7 - 10 days (6).
3.2 All CVL must be inserted with strict aseptic technique according to local WoS guidelines. The line tip position must be adequately confirmed (32-37) prior to the infusion of PN.
3.3 Catheter-related blood stream infection is the most common complication related to central venous access therefore meticulous attention to line sterility is vital. Access to the line should be minimised and ideally the line should be used solely for PN although this may be impractical due to difficulties in venous access. If other infusions do need to run alongside the PN multi lumen extension lines should be used, with all crystalloid infusions passing through the antibacterial pre-filter. Compatibility must be confirmed using the appropriate IV drug monograph or in discussion with pharmacy (6).
3.4 Peripheral venous catheters may be used for short term PN administration. Only use peripheral venous access to give PN if it would avoid a delay in starting PN or short term is anticipated (<5 days) or if central venous access is impractical. In this situation the maximum osmolality should ideally be 1425mOsm/L (6) The standard bag (12.5%) has an Osmolality of 1080mOsm/L when run alone and a total osmolality of 958mOsm/L when run with lipid. PN that is not suitable for peripheral line administration must be clearly labelled: ‘to be given by central line only’ e.g. bags with higher glucose concentrations, and /or additions of potassium and calcium. (4).
3.5 Additions to PN solutions must only be made on a PAU. NO Additions to PN should be made at ward level. Any manipulation of electrolytes felt to be necessary must be discussed and approved by the attending consultant and then given as separate infusions according to the information in section 2.2 / appropriate IV monograph/ local protocol. Any changes made to the PN regimen must be recorded for audit purposes.
3.6 There is some evidence that light exposure increases the products of oxidation in both aqueous and lipid PN and that this may contribute to increased oxidative stress in preterm infants (21). Light protection has been shown to decrease the accumulation of triglycerides in plasma and may allow for higher rates of lipid infusion and improved nutrition. Light protection may also help to prevent vitamin degradation.
Where possible amber syringes should be used for lipid administration, or bags / bottle of lipid covered with a light protective cover, and a light protective line also used. The aqueous component of the PN regimen should also be covered with a light protective cover.
3.7 Aqueous PN solutions with 0.22 micron filters can be infused over 48 hours in stable neonates. Lipid infusions should initially be infused over 24 hours as this has been shown to improve lipid tolerance in preterm infants without adversely affecting lipid monitoring, and changed every 24 hours.. Cycling over 20 hours may be indicated in certain patients (see Table 3)
3.8 Lipid with added water and fat soluble vitamins is given as a separate infusion to the aqueous component of PN, although both infusions can be administered through the same line (via a y site).
3.9 Each unit must make arrangements for pre-prepared PN (both aqueous solutions and lipid emulsions) to be available 24 hours a day (4) to ensure that all infants meeting the criteria can be commenced on PN as early as possible (10).
3.10 PN should always be infused via in-line filters; 0.22 micron hydrophilic filters for aqueous PN and 1.2 - 1.5 micron hydrophobic filters for lipid emulsions (7).
3.11 The giving set and filters must be changed every 48 - 96 hours as per manufacturer’s instructions for aqueous PN and every 24 hours for lipid.
3.12 PN infusion set up, attachment of the giving set and connection to the patient should be performed using full aseptic non-touch technique (ANTT).
3.13 The PN infusions supplied by pharmacy contain an overage (an additional volume of fluid) to allow the priming of the giving sets without reducing the volume available for infusion into the patient. Local policy will determine what documentation is supplied with the bag.
The plastic outer bag in which the PN is supplied is simply protective and is not a sterility barrier.
3.14 Checking - all TPN should be checked against prescription and fluid requirements by two registered nurses, one of whom must be qualified in speciality. Both nurses to remain present until PN infusions are set up in infusion devices and lines are connected to the patient. A final safety check at the point of administration of PN should be performed including checking the labels of PN solutions (aqueous and lipid) against the pharmacy prescription form and the PN / fluid chart for:
- Name of patient and hospital / CHI number
- Route of administration (central or peripheral)
- Date of infusion
- Rate of infusion
- Expiry
- Doses of all ingredients prescribed (check label against prescription) if this detail is on the prescription
- Appearance of the parenteral nutrition solutions
3.15 All nurses who commence PN infusions should be trained in ANTT and IV management and receive appropriate updates.
Training records should be kept for all nurses to demonstrate individual competence.
4.0 Weaning of PN
4.1 Enteral feeding should be introduced according to the WoS Enteral Feeding Guideline. Once enteral feed volumes increase beyond trophic feeds (24 ml/kg/day) and are being tolerated they should be considered when prescribing PN volumes.
4.2 As enteral feeds increase PN should be reduced accordingly (6). Both the aqueous and the lipid components should be reduced proportionately to the increase in enteral feeds.
As enteral feeds commence, lipids can continue as long as levels are OK until a decision is made to stop them or to wean.
As enteral feeds commence, lipids in the milk replace IV lipids. As a general rule:
- Quarter of the fluid intake is milk à reduce IV lipid to 3 g/kg/day
- Half of the fluid intake is milk à reduce IV lipid to 2g/kg/day
- Three quarters of fluid intake is milk à reduce lV lipid to 1g/kg/day
4.3 PN should be continued until at least 120ml/kg/day of enteral feed is tolerated. For babies born before 28+0 weeks, consider continuing parenteral nutrition until the enteral feed volume is 140 to 150 ml/kg/day. Many preterm infants will need to continue increments in enteral feed volumes to a total combined feed volume of >150ml/kg as long as there are no clinical contraindications.
Standard Formulation – 12.5% glucose with lipid
Standard Formulation – 10% glucose with lipid
Sodium Free Formulation with lipid
Central line Formulation – 15% glucose with lipid
Totals per 100ml of aqueous PN
Standard Formulation – 12.5% glucose with lipid
|
|
75ml/kg/d |
90ml/kg/d |
105ml/kg/d |
120ml/kg/d |
135ml/kg/d |
150ml/kg/d |
|
Protein (g/kg/day) |
1.78 |
2.26 |
2.53 |
2.94 |
3.35 |
3.55 |
|
Amino Acid (g/kg/day) |
2 |
2.5 |
2.8 |
3.3 |
3.8 |
4 |
|
Sodium (mmol/kg/day) |
2 |
2.46 |
2.77 |
3.3 |
3.8 |
4.2 |
|
Potassium (mmol/kg/day) |
0.82 |
1.01 |
1.14 |
1.34 |
1.5 |
1.66 |
|
Phosphate (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
1.88 |
2 |
|
Calcium (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
1.88 |
2 |
|
Magnesium (mmol/kg/day) |
0.11 |
0.13 |
0.15 |
0.18 |
0.2 |
0.22 |
|
Glucose (12.5%)(g/kg/day) |
7.88 |
9.75 |
11 |
12.88 |
14.75 |
16 |
|
Lipid (g/kg/day) |
2 |
2 |
3 |
3 |
3.5 |
3.5 |
|
Energy (Kcal/kg/day) |
52 |
59 |
74 |
82 |
89 |
100 |
Standard Formulation – 10% glucose with lipid
|
|
75ml/kg/d |
90ml/kg/d |
105ml/kg/d |
120ml/kg/d |
135ml/kg/d |
150ml/kg/d |
|
Protein (g/kg/day) |
1.65 |
2.05 |
2.31 |
2.7 |
3.03 |
3.43 |
|
Amino Acid (g/kg/day) |
1.9 |
2.3 |
2.6 |
3 |
3.4 |
3.9 |
|
Sodium (mmol/kg/day) |
2 |
2.46 |
2.77 |
3.3 |
3.8 |
4.2 |
|
Potassium (mmol/kg/day) |
0.82 |
1.01 |
1.14 |
1.34 |
1.5 |
1.66 |
|
Phosphate (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
1.88 |
2 |
|
Calcium (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
1.88 |
2 |
|
Magnesium (mmol/kg/day) |
0.11 |
0.13 |
0.15 |
0.18 |
0.2 |
0.22 |
|
Glucose (10%)(g/kg/day) |
6.3 |
7.8 |
8.8 |
10.3 |
11.55 |
13 |
|
Lipid (g/kg/day) |
2 |
2 |
3 |
3 |
3.5 |
3.5 |
|
Energy (Kcal/kg/day) |
45 |
51 |
65 |
71 |
81 |
87 |
Sodium Free Formulation with lipid
|
|
75ml/kg/d |
90ml/kg/d |
105ml/kg/d |
120ml/kg/d |
135ml/kg/d |
150ml/kg/d |
|
Protein (g/kg/day) |
1.43 |
1.78 |
2 |
2.33 |
2.66 |
2.96 |
|
Amino Acid (g/kg/day) |
1.61 |
2 |
2.26 |
2.62 |
3 |
3.33 |
|
Sodium (mmol/kg/day) |
0 |
0 |
0 |
0 |
0 |
0 |
|
Potassium (mmol/kg/day) |
1.02 |
1.26 |
1.41 |
1.65 |
1.86 |
2.07 |
|
Phosphate (mmol/kg/day) |
0.38 |
0.47 |
0.53 |
0.61 |
0.69 |
0.78 |
|
Calcium (mmol/kg/day) |
0.38 |
0.47 |
0.53 |
0.61 |
0.69 |
0.78 |
|
Magnesium (mmol/kg/day) |
0.11 |
0.13 |
0.15 |
0.17 |
0.2 |
0.22 |
|
Glucose (10%)(g/kg/day) |
6.3 |
7.8 |
8.7 |
10.2 |
11.5 |
12.8 |
|
Lipid (g/kg/day) |
2 |
2 |
3 |
3 |
3.5 |
3.5 |
|
Energy (Kcal/kg/day) |
45 |
51 |
65 |
71 |
81 |
87 |
Central line Formulation – 15% glucose with lipid
|
|
75ml/kg/d |
90ml/kg/d |
105ml/kg/d |
120ml/kg/d |
|
Protein (g/kg/day) |
1.78 |
2.26 |
2.53 |
2.94 |
|
Amino Acid (g/kg/day) |
2 |
2.5 |
2.8 |
3.3 |
|
Sodium (mmol/kg/day) |
2 |
2.46 |
2.77 |
3.3 |
|
Potassium (mmol/kg/day) |
0.82 |
1.01 |
1.14 |
1.34 |
|
Phosphate (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
|
Calcium (mmol/kg/day) |
1 |
1.27 |
1.42 |
1.65 |
|
Magnesium (mmol/kg/day) |
0.11 |
0.13 |
0.15 |
0.18 |
|
Glucose (15%)(g/kg/day) |
9.43 |
11.7 |
13.2 |
15.45 |
|
Lipid (g/kg/day) |
2 |
2 |
3 |
3 |
|
Energy (Kcal/kg/day) |
58 |
67 |
83 |
92 |
NB: Maximum volumes for this bag (including lipid) is 123ml/kg/day (maximum total glucose dose)
All Bags
- Vitlipid N Infant / Solivito/ Peditrace as per recommended prescription doses
Totals per 100ml of aqueous PN
|
|
Standard bag 10% |
Standard bag 12.5% |
Central bag 15% |
Sodium free bag 10% |
|
Protein (g) |
2.6 |
2.88 |
2.88 |
2.27 |
|
Amino Acid (g/kg/day) |
2.9 |
3.2 |
3.2 |
2.56 |
|
Sodium (mmol) |
3.2 |
3.2 |
3.2 |
0 |
|
Potassium (mmol) |
1.31 |
1.31 |
1.31 |
1.62 |
|
Phosphate (mmol) |
1.62 |
1.62 |
1.62 |
0.6 |
|
Calcium (mmol) |
1.62 |
1.62 |
1.62 |
0.6 |
|
Magnesium (mmol) |
0.17 |
0.17 |
0.17 |
0.17 |
|
Glucose (g) |
10 |
12.5 |
15 |
10 |
|
Energy (Kcal) |
40 |
50 |
60 |
40 |
West of Scotland Parenteral Nutrition Guideline
Which bag do I choose for a preterm infant?
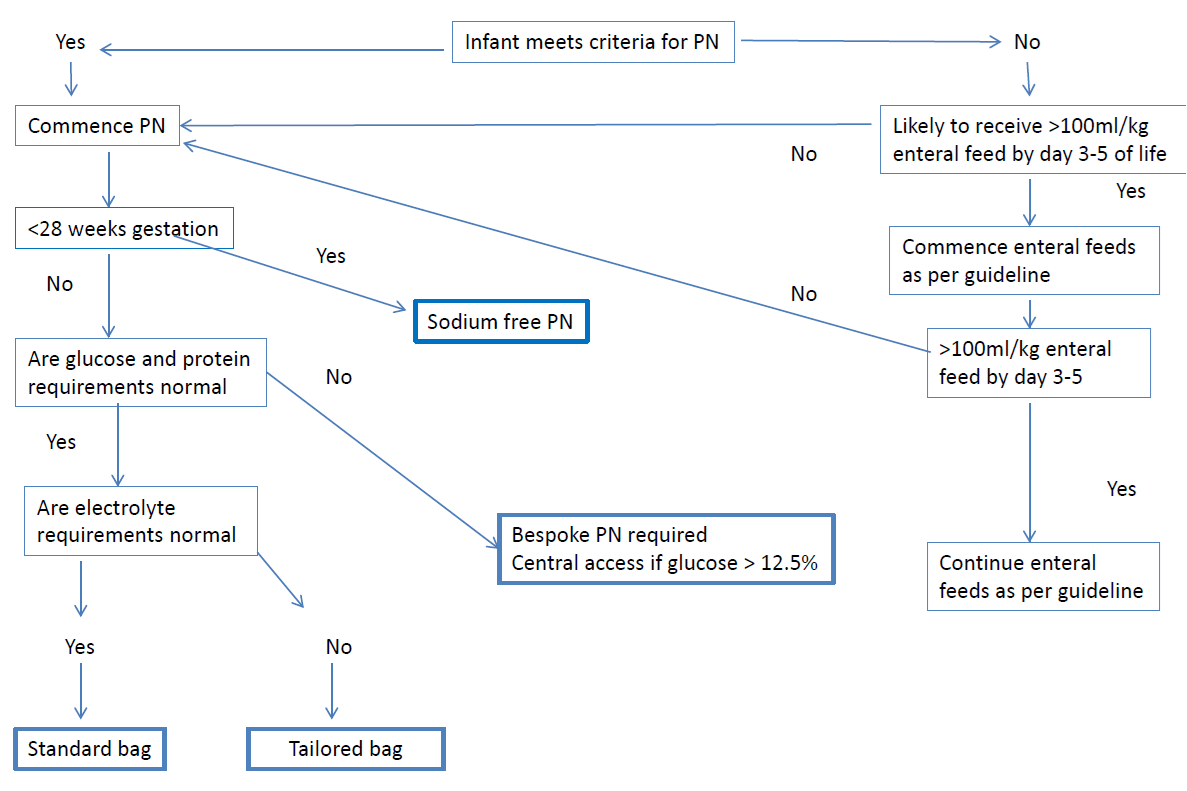
- 100% infants meeting the absolute indicators within the prescribing criteria commence parenteral nutrition within 6 hours of birth.
- 100% infants meeting prescribing criteria receive a minimum of 2g/kg/day amino acid on day 1 of PN.
- 100% infants have PN accurately prescribed using the West of Scotland Standardised PN prescribing proforma.
- No manipulations to PN solutions at ward level
- All blood sugars levels documented on daily chart
- Insulin infusion commenced
- Babies continued on PN after reaching relevant volume of tolerated enteral feeds