
Emergency contraception
exp date isn't null, but text field is
Objectives
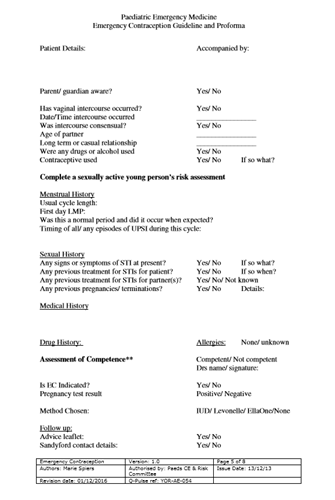
Indications, exclusions and methods of emergency contraception available for adolescents. This includes information about the assessment of failure or potential failure of a contraceptive method. A proforma and algorithm are supplied to aid a healthcare professional.
Scope
Adolescents requiring emergency contraception advice.
Audience
Medical and nursing staff involved in the assessment, delivery of advice and management of young people requiring emergency contraception.
November 2023: This guidance is currently under review as it has gone beyond the standard review date. It reflects best practice at the time of authorship / last review and remains safe for use. If there are any concerns regarding the content then please consult with senior clinical staff to confirm.
Please read in conjunction with Managing sexually active young people - staff guidance
Indications
- Unprotected sexual intercourse (UPSI)
- Failure or potential failure of contraceptive method*
- Wish to reduce likelihood of pregnancy
Not Indicated if:
- Positive pregnancy test
- More than one episode of UPSI this cycle, the first of which is greater than 120 hours ago
Copper IUD
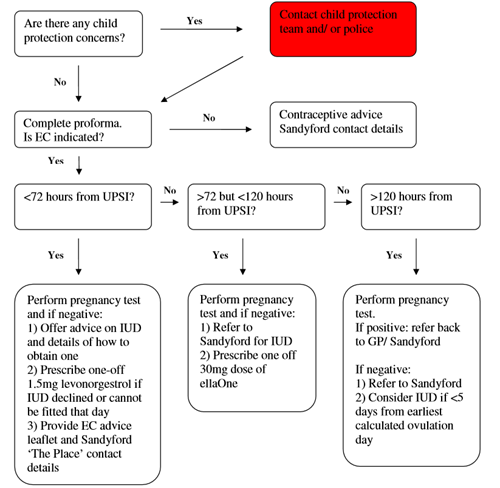
- IUD advice and Sandyford contact details should be offered to all females presenting for EC as this is the most effective method to prevent pregnancy
- If used, ideally should be fitted at first presentation. POEC should be given in addition if a future appointment is made for IUD insertion
- Effective up to 120 hours (5 days) of UPSI in current cycle
- If UPSI >120 hours an IUD can be fitted up to 5 days after earliest calculated day of ovulation
- Estimated failure rate 0.1%
- Prophylactic antibiotics to cover Chlamydia required at time of insertion if female thought to be at risk
Progestogen only EC (POEC) - Levonelle 1500
- 1.5mg levonorgestrol one off dose taken as soon as possible within 72 hours UPSI
- Prevents 86% of expected pregnancies
- Efficacy may be affected the later treatment is given following UPSI
- Side effects include- nausea, vomiting, dizziness, headache, lethargy, abdominal pain, breast tenderness and irregular periods
- Offer domperidone if nausea/ vomiting has been experienced with previous use
- Repeat dose indicated if vomiting occurs within 2 hours
- Drug interactions with liver enzyme inducing drugs e.g. St John’s Wort, second dose should be given 12 hours later
- No absolute medical contraindications
- Caution with wafarin
- Abstinence/ consistent and correct barrier method required for the rest of the cycle
- Does not protect against pregnancy for the rest of the cycle
- Follow up if period does not start within three weeks or differs significantly from normal should be advised
Ulipristal- ellaOne
- Progesterone receptor modulator
- Single 30mg dose licensed for use up to 120 hours after UPSI, not licensed for use in under 18s but use in this age group is supported by the Faculty of Sexual and Reproductive Health
- EllaOne should NOT be more than once in a cycle
- Contraindicated in: pregnancy, uncontrolled asthma or severe liver disease
- Side effects include: abdominal pain and menstrual disturbances
- Efficacy may be reduced in patients taking liver enzyme inducing drugs and drugs that increase gastric pH
- Can reduce the effectiveness of combined-hormonal (COCP) and progesterone only (POP) contraceptive - additional precautions required for 14 days (or until next period)
Combined pill (COCP)
- One pill missed at any time:
- Take most recent missed pill as soon as remembered
- Continue to take remaining pills at usual time
- No additional contraception required
- EC not required
- Two or more pills missed at any time:
- Take most recent pill as soon as remembered
- Continue to take remaining pills at usual time
- Additional contraception/ abstinence until pill taken correctly for 7 days
In addition:
- If pills are missed day 1-7, consider EC if UPSI has occurred in the pill free interval or day 1-7
- If pills are missed day 15-21, pill free interval should be omitted (e.g. two packs run together with no break)
- EC indicated if UPSI/ failed barrier method with 28 days following use of liver enzyme inducing drugs
Progestogen Only Pill (POP)
- One or more pills missed or >3 hours late (12 hours for Cerazette) and UPSI has occurred in the 2 days following missed pill then EC is indicated
- Additional contraception/ abstinence required until pill has been taken correctly for 2 days
- EC indicated if UPSI/ failed barrier method with 28 days following use of liver enzyme inducing drugs
Barrier methods
- Condom rupture/ slippage/ misuse or not used
- Diaphragm/ cap incorrectly inserted/ dislodged/ torn
Copper IUD/Mirena Coil
- Complete or partial expulsion is identified EC is required
- If removal of normally sited device is required EC should be offered if UPSI had occurred in the last 7 days
Depo-Provera
- EC indicated if contraceptive injection is late (i.e. more that 14 weeks from last injection) and UPSI has occurred
Progestogen only implants
- EC indicated if UPSI/ failed barrier method has occurred during or in the 28 days following liver enzyme inducing drugs

|
Discharge and Follow up: All cases should be provided with an EC leaflet: Click here for leaflet All cases should be given contact details for the Sandyford ‘The Place’ clinic: Click here for website Advise to seek medical attention if:
|
1. West of Scotland Sexual Health Managed Clinical Network
2. FSRH Clinical Guidance. Emergency contraception December 2017
3. FSRH Missed Pills Recommendations May 2011
4. FPA: Your guide to emergency contraception leaflet March 2011
Last reviewed: 13 December 2013
Next review: 30 April 2024
Author(s): Dr Marie Speirs
Approved By: Clinical Effectiveness
Document Id: 117