
Feverish Illness in Children (< 5 years) Paediatric Emergency Department, RHC
exp date isn't null, but text field is
November 2023: This guidance is currently under review as it has gone beyond the standard review date. It reflects best practice at the time of authorship / last review and remains safe for use. If there are any concerns regarding the content then please consult with senior clinical staff to confirm.
Introduction
Feverish illness is a common occurrence in childhood. It is the most frequent reason for parents to consult a doctor about their child, and is the second most common cause of hospital admission in childhood.1 Most are self-limiting, however despite this, infections are the most common cause of death in those aged less than 5 years.1 Therefore it is important to identify those with potentially severe infections and initiate treatment rapidly.
Feverish Illness is diagnosed in all children (<5years) who present with a temperature over 38°C as measured by the following as advised by NICE guidelines1
- In those <4weeks of age – electronic thermometer placed in axilla
- In those >4 weeks of age
- Chemical dot in axilla
- Electronic thermometer in axilla
- Infra-red tympanic thermometer
- In addition this includes those children who have no recorded fever at triage or assessment but whose parents report fever at home
- regular temperatures should be taken whilst in the ED to monitor for this
Observations
All children who present with fever/parental reports of fever at home should have the following recorded at triage1
- HR
- BP (if HR is recorded as abnormal)
- RR
- Oxygen saturations
- Temperature
- CRT (centrally and peripherally)
- Presence of a non-blanching rash
- History of recent foreign travel recorded
- Immunisation history
In addition, parents should be given urine kit, and asked to collect sample for analysis.
Those children who have any ABC compromise, appear ill to health care professional, or have markedly deranged physiology should be taken immediately to the resuscitation area and a senior doctor should be involved. Treat according to APLS guidance 1,2
The remaining children should continue to be triaged appropriately and if pyrexia is present, one anti-pyretic agent should be administered if not already done so prior to presentation, doses of which can be found in the BNFc3
If ABC compromise/ill looking child/markedly deranged physiology the child should be taken to resus and managed according to APLS guidance2
The following should be assessed and documented in all feverish children1
- History of illness and any features of specific disease (e.g. tonsillitis, UTI)
- Full examination of child including ENT, inspection of all joints, hernial orifices and exposure of all skin areas.
- Hydration and circulation status – CRT, extremity temperatures, presence of peripheral pulses, skin turgor, mucus membranes
- Appearance of skin (e.g. mottled, pale, pink)
- Activity levels
- Respiratory pattern
- Signs of severe illness (non-blanching rash, prolonged fever, neurological signs)
These children should then be assigned to a colour group in keeping with the NICE guidance on feverish children” 2013’s traffic light system1. This will help determine further management.
Children will be classified into either into GREEN, AMBER or RED groups depending on their clinical assessment.1 Re-assess the child once anti-pyretic medications have been administered as this may alleviate some clinical features and the child may be grouped into a lower severity group.
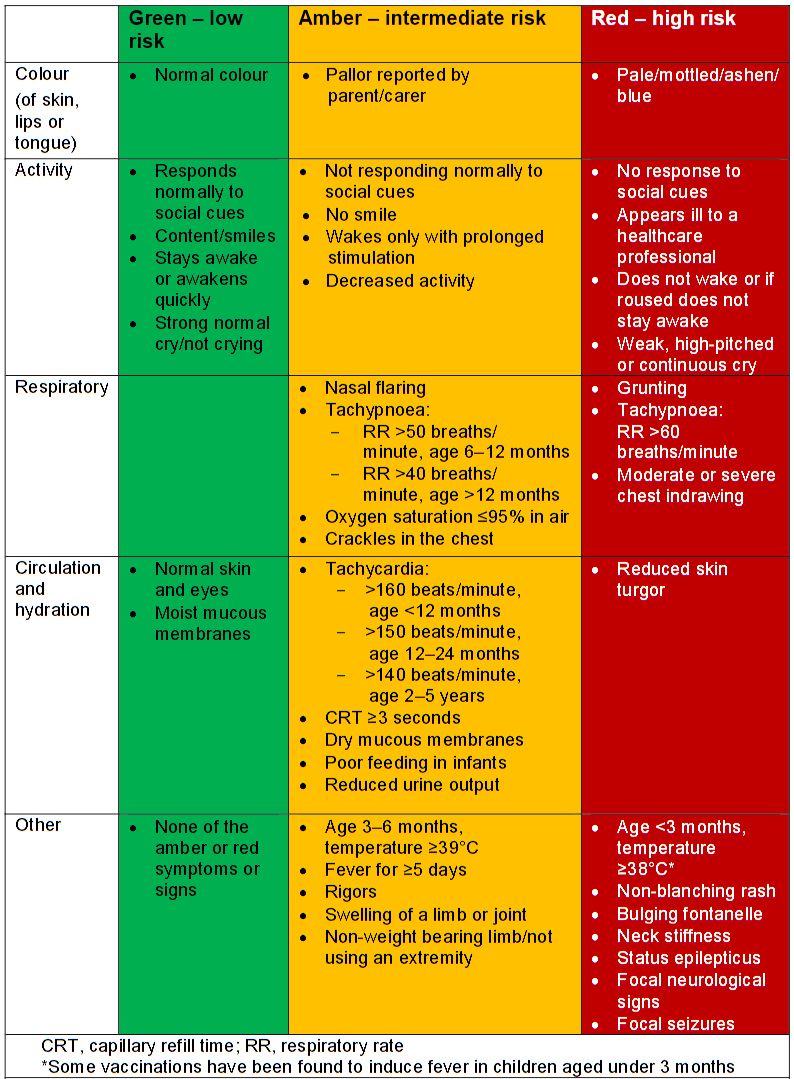
Figure 1: Table taken from NICE Clinical Guideline 160 - Feverish illness in children 2013.
Children under 1 month
ALL children under 1 month of age with a documented fever >38° or those that appear unwell should undergo a full septic screen which should consist of:
- Bloods including blood cultures
- Urine microscopy, culture and sensitivity
- LP*
- CXR
IV antibiotics should be given in accordance with local guidelines.
*Please see RHSC lumbar puncture guideline for contraindications to LP
Children under 3 months of age1
- with documented fever in ED
OR - apyrexial on assessment but who have parental reports of fever at home
OR - no documented fever but appear unwell on examination
in whom no apparent source is found, the following investigations are advised1, and the patient should be admitted under medical paediatrics.
- FBC
- Blood Culture
- CRP
- Urinalysis and CSU
- CXR on clinical judgement
- LP* should be performed on the majority of children in this age group, unless there is a clear reason not to do so and this has been discussed with a senior clinician.
Administer IV antibiotics (refer to local guidance) if
- 1-3months who appear unwell
- If WCC <5x109/L or >15x109/L
In addition, children <3 months who have fever with a clear source should be discussed with the ED consultant on duty or medical registrar out of hours for admission to CDU or ARU for an extended period of monitoring +/- further investigation.
Children > 3 months of age1
- if a source is identified then management should be directed towards that specific illness
- If no source is found then management should be directed as per NICE traffic light system, described below1
| RED1 | |||
|
IMPORTANT These children are likely to be septic, and should be managed with the early input of a senior clinician and early administration of IV antibiotics considered. |
||
| AMBER1 | |
|
|
| GREEN1 | |
|
|
Children with a clear source of infection should be treated appropriately as per local guidance specific to that febrile illness, with written and verbal advice given to parents.
Children in the green category with no clear cause of pyrexia may be discharged home after assessment and appropriate investigations are completed. There should be a responsible adult at home and parental anxiety should be addressed.
Children not deemed suitable for discharge home after ED assessment should be admitted either to the CDU or directly to the ARU, following discussion with the senior doctor on the ED floor.
Advice sheet for parents (pdf):
- National Institute for Health and Care Excellence (2013) Feverish illness in children. [160]. London: National Institute for Health and Care Excellence
- Advanced Paediatric Life Support The Practical Approach (2005) 5th Edition, ALSG group. Wiley and Sons, Oxford.
- Joint Formulary Committee British National Formulary For Children. 55th Ed., London: British Medical Association and Royal Pharmaceutical Society of Great Britain. Joint Formulary Committee (2013) British National Formulary.
Last reviewed: 23 October 2018
Next review: 30 April 2024
Author(s): Marie Spiers
Version: 2
Approved By: Paediatric & Neonatal Clinical Risk & Effectiveness Committee