
Ingested foreign bodies, Emergency Department
exp date isn't null, but text field is
Objectives
*** IF SUSPECTED OR KNOWN INGESTION OF BUTTON BATTERY &/OR MAGNET(S) THEN DISCUSS WITH ED SENIOR IMMEDIATELY***
Guidance for the assessment and management of ingested foreign bodies, including a management algorithm.
Scope
Children that have ingested a foreign body.
Audience
Medical and nursing staff in the Emergency Department.
November 2023: This guidance is currently under review as it has gone beyond the standard review date. It reflects best practice at the time of authorship / last review and remains safe for use. If there are any concerns regarding the content then please consult with senior clinical staff to confirm.
*** IF SUSPECTED OR KNOWN INGESTION OF BUTTON BATTERY &/OR MAGNET(S) THEN DISCUSS WITH ED SENIOR IMMEDIATELY ***
History of foreign body ingestion is a common presenting complaint. Metallic foreign bodies are more commonly implicated than non-metallic. Coins are the most common.
Most ingested foreign bodies will pass harmlessly through the GI tract. However oesophageal impaction is a recognised complication even in the asymptomatic [1] with potentially serious sequelae such as oesophageal perforation, mediastinitis and ulceration.
Metal detectors have been used to detect metal foreign bodies in several studies. They have been proven to be both sensitive and specific in confirming presence of coins in particular, and localising them to above or below the diaphragm [2].
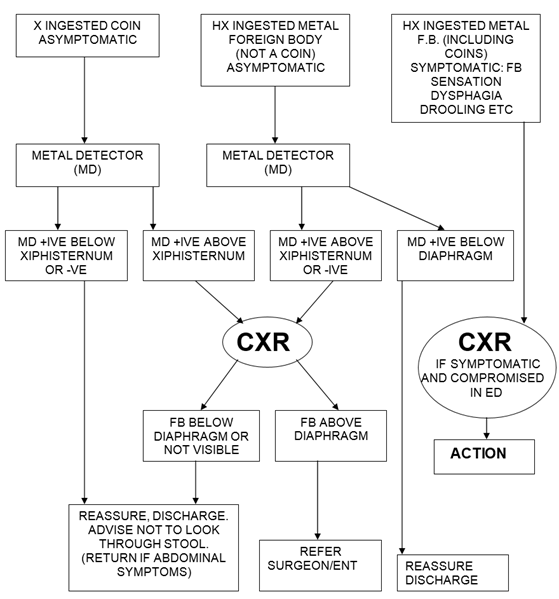
- In children who have a history of swallowing a radiolucent FB and are asymptomatic with normal examination reassure and discharge with advice to return if significant symptoms appear.
- In children who have a history of swallowing a radiolucent FB who are symptomatic i.e. drooling, FB sensation, dysphagia refer surgical team.
- For metallic FB see flow chart below. Good evidence exists for localisation of coins with a metal detector. The evidence for non-coin metal FBs is not as strong so if metal detection were negative we would advise confirmation with a CXR.
- If FB metal detector positive above diaphragm but not visible on CXR retry with metal detector. Consider aluminium FB (radiolucent).
- Several case studies have highlighted the danger of swallowing multiple mini magnets (used on notice boards etc).
- Sharp objects should be treated in the same way as other metal foreign bodies although complication rates increase from less than 1% to 15 to 30%
1. Litovitz T & Schmitz BF. (1992) Ingestion of cylindrical and button batteries: an analysis of 2382 cases. Pediatrics 89, pp. 747–757. [NOTE: contact knowledge@nes.scot.nhs.uk quoting your Athens username to receive the publisher password for this journal]
2. Lee JB, Ahmad S, & C P Gale CP. (2005). Detection of coins ingested by children using a handheld metal detector: a systematic review. Emerg. Med. J. 22: 839 - 844.
3. Choudhery V & Maurice S. (2000) BEST EVIDENCE TOPIC REPORTS: Signs and symptoms of oesophageal coins. Emerg. Med. J., Mar 2000; 17: 126 – 127.
Last reviewed: 24 February 2017
Next review: 01 December 2023
Author(s): Steve Foster
Approved By: Clinical Effectiveness