
Management of failing Hickman Line for pulmonary hypertension patients on IV Epoprostenol infusion
exp date isn't null, but text field is
Objectives
To provide a guideline for the management of a blocked, broken or infected central line in a paediatric patient receiving a continuous infusion of intravenous Epoprostenol for the treatment of pulmonary arterial hypertension.
Scope
This guideline is intended for all healthcare professionals involved in the care of paediatric patients with pulmonary arterial hypertension receiving a continuous infusion of Epoprostenol.
Pulmonary arterial hypertension is a relatively rare condition in the paediatric population and is associated with diverse diseases with onset at any age. It is characterized by pulmonary vascular remodelling leading to elevated pulmonary arterial pressure and, over time, right ventricular dysfunction, under filling/compression of the left ventricle, and terminal heart failure. It is defined as a mean pulmonary artery pressure of > 20 mmHg, measured by cardiac catheterisation.
Treatment for children classified in the high risk groups (WHO functional class III-IV) is a continuous infusion of intravenous Epoprostenol via a central line. This is a life supporting continuous infusion, with a very short half-life of 2-3 minutes. An interruption of Epoprostenol infusion may precipitate a pulmonary hypertensive crisis.
Epoprostenol mechanisms of action:
- Potent vasodilator of pulmonary and systemic vascular arterial beds
- Inhibits platelet aggregation
- Slows the process of scarring and rapid growth of new cells in long vessels
The haemodynamic effects of Epoprostenol include reduced pulmonary vascular resistance, increased cardiac index, and increased oxygen delivery. However, hypotension is also a haemodynamic effect.
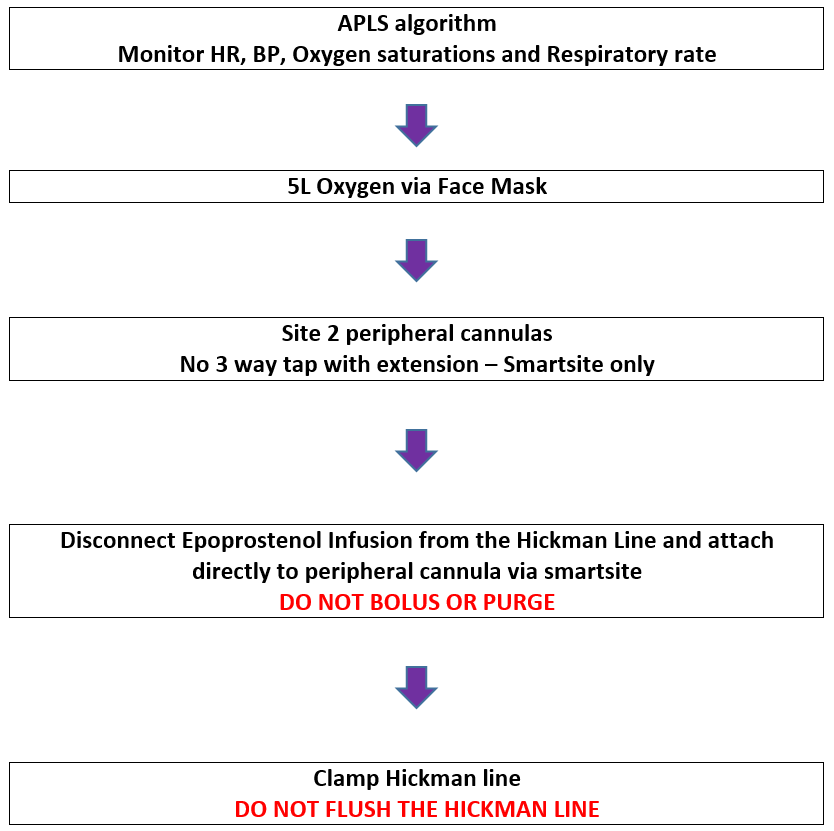
Please refer to Flowchart 2 for ongoing management
![]()
![]()
CADD Pump
Parent remain resident on ward 1e and are responsible for pump (suitable for short term in patient stay)
Alaris syringe driver
Parent not resident on ward 1e. Infusion to be given via an Alaris syringe driver as ward nurses not trained in CADD pump. Nursing staff responsible for syringe driver. Parents will make up a 50 ml infusion in a syringe compatible with Alaris pump
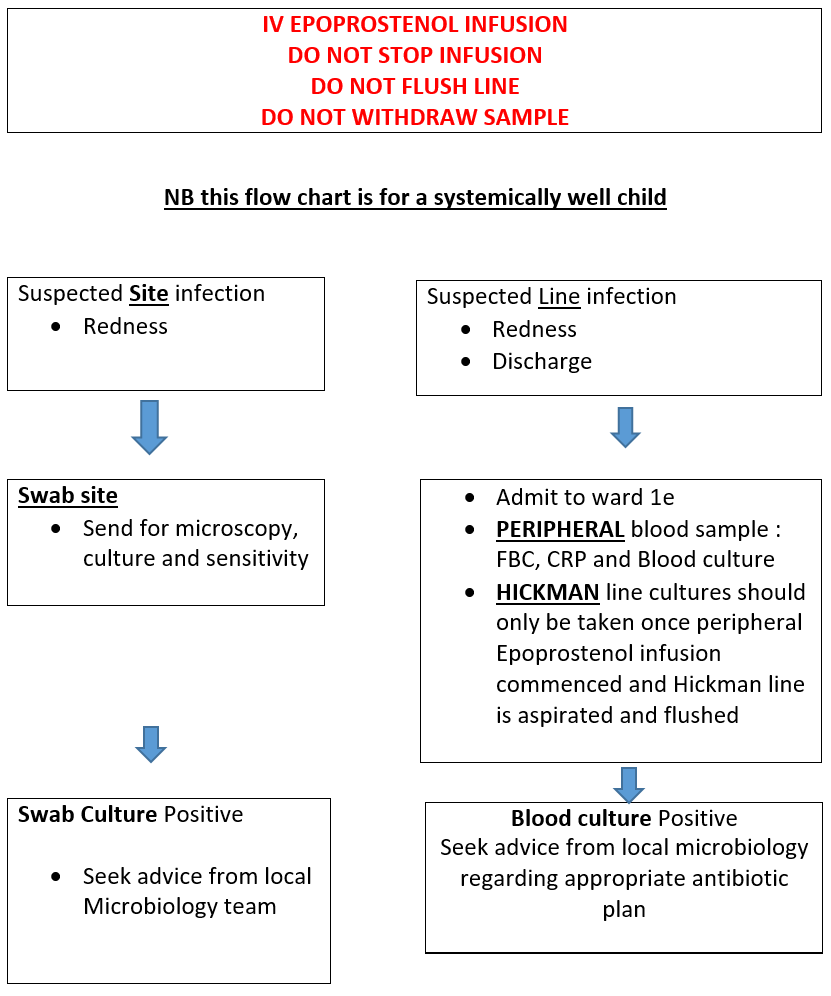
- Great Ormond Street Hospital. Management of Hickman line infection. (Online). London: Great Ormond street Hospital NHS Trust (Accessed 1st February 2022)
- Great Ormond Street Hospital. Transition from Hickman line to peripheral line. (Online). London: Great Ormond street Hospital NHS Trust (Accessed 1st February 2022)
- Great Ormond Street Hospital. Transition from peripheral line to Hickman line. (Online). London: Great Ormond street Hospital NHS Trust (Accessed 1st February 2022)
- Starship Child Health. Epoprostenol (Veletri) for paediatric cardiology. (Online). Auckland: Starship Child Health. (Accessed 20th December 2022). Available from Epoprostenol (Veletri®) for paediatric cardiology (starship.org.nz)
Last reviewed: 07 November 2023
Next review: 30 November 2026
Author(s): Claire Cairney, Cardiac Nurse Specialist, Alison Buller Cardiac ANP
Version: 1
Co-Author(s): Adapted from the Starship Children’s Hospital, Auckland, NZ and Great Ormond Street Hospital, London, UK guidelines
Approved By: Cardiac Guideline Group